Brian Sowka, DO, Padmavathi Mali, MD, Milan Folkers, MD Gundersen Health System, La Crosse, WI
Introduction: Plasmablastic lymphoma occurring in the gastrointestinal tract represents a rare malignancy in gastroenterology and has an unknown prevalence. There are only a handful of cases in the literature in which this rare malignancy presents in the GI tract, typically in patients who have preexisting immunosuppression. Here we present a patient with known Barrett’s esophagus who was found to have plasmablastic lymphoma of the distal esophagus.
Case Description/Methods: A 54 year old white male with history of Barrett’s esophagus, presbyesophagus, GERD with hiatal hernia, adenomatous polyps, cerebral palsy, Factor V Leiden heterozygous, and seizure disorder presented to his primary care clinic for several months of progressive dysphagia, nausea, emesis, and functional decline. His Barrett’s esophagus had been present for at least 9 years undergoing regular surveillance without evidence of dysplasia. His labs showed a normocytic anemia and significantly elevated ESR and CRP. A CT scan of the chest, abdomen, pelvis was performed which revealed thickening of distal third of the esophagus, 2.7 cm necrotic paraesophageal lymph node, and multiple enlarged lymph nodes in the gastric hepatic ligament. The patient underwent EGD with EUS which revealed a tumor in the distal third of esophagus. Multiple biopsies were taken which showed necrotic plasmablastic lymphoma, non-dysplastic Barrett’s mucosa positive for CD10, CD138, MIB-1, epithelial membrane antigen, and weakly positive for PAX-5, CD45, CD56. The patient underwent additional evaluation by oncology and was started on EPOCH chemotherapy. HIV testing returned negative. Unfortunately the malignancy progressed despite chemotherapy and radiation and the patient died about 5 months after initial diagnosis.
Discussion: Plasmablastic lymphoma represents a rare, aggressive subtype of diffuse large B-cell lymphomas. Typical organs involved include the GI tract, lymph nodes, oral mucosa, and skin. Unfortunately the disease course relapses frequently and is refractory to chemotherapy. It is more prevalent in patients with immunocompromised states including patients with inflammatory bowel disease, HIV, or EBV. However, in our patient this malignancy arose in the setting of Barrett’s esophagus previously without dysplasia or prior HIV, EBV infections. We suggest this rare diagnosis be in the differential in patients undergoing evaluation of esophageal masses.
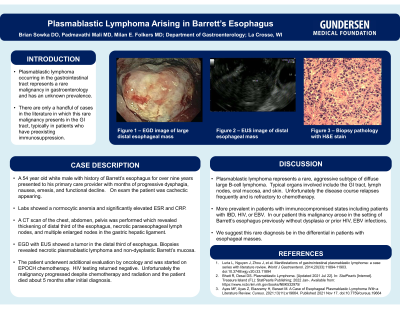
Figure: A – EGD image of large distal esophageal mass B – EUS image of distal esophageal mass C – Biopsy pathology with H&E stain
Disclosures:
Brian Sowka indicated no relevant financial relationships.
Padmavathi Mali indicated no relevant financial relationships.
Milan Folkers indicated no relevant financial relationships.
Brian Sowka, DO, Padmavathi Mali, MD, Milan Folkers, MD. A0237 - Plasmablastic Lymphoma Arising in Barrett’s Esophagus: A Case Report, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.