Thomas R. Checketts, DO1, Manjushree Gautam, MD2, Steven A. Mudrovich, MD3, Stevan A. Gonzalez, MD4 1Creighton University, Papillion, NE; 2Liver Consultants of Texas, Fort Worth, TX; 3Baylor All Saints Fort Worth, Fort Worth, TX; 4Baylor Simmons Transplant Institute, Fort Worth, TX
Introduction: Duodenal follicular lymphoma (DFL) are uncommon, only being recognized as a new entity by the World Health Organization (WHO) in 2016. Over a 39-year period, the Surveillance, Epidemiology, and End Results (SEER) registry only found 1109 cases. Detection of lesions occurs in both symptomatic and asymptomatic patients. Treatment options include surgery, radiation, chemotherapy (including rituximab) and varying combinations. Curiously, many patients do very well with little to no treatment. At five years, progression-free survival is greater than 70% and overall survival ranges from 80-94%. A better understanding of the characteristics of FL of the GI tract relating to epidemiology, pathophysiology, treatment options, and long-term outcomes is needed.
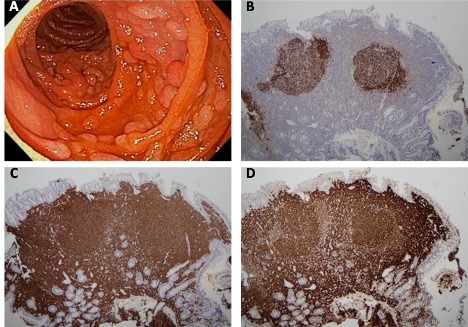
Case Description/Methods: A 57-year-old female with nonalcoholic steatohepatitis (NASH) cirrhosis underwent upper endoscopy surveillance for gastroesophageal varices. For the year prior, the patient reported a poor appetite and 30-pound weight loss. She denied any personal or family history of malignancy. She otherwise reported no gastrointestinal symptoms. Endoscopic evaluation revealed multiple small round polyps in a diffuse distribution in the second portion of the duodenum (Figure A). Tissue in-situ hybridization was positive for BCL2/IGH fusion loci establishing a diagnosis of follicular B-cell lymphoma. Immunohistochemical staining patterns and morphology indicated a low-grade lesion (Figures B-D). Further work up included PET/CT, which was negative for systemic disease. Based on the indolent natural history of DFL, plans are for observation.
Discussion: Stage I/II gastrointestinal FL (GI-FL) are associated with >80% 5-year survival. Many of these patients do not require treatment. Given its rarity, little is known about its pathogenesis. DFL shows a female predilection in as high as a 2:1 ratio. The most common location is in the duodenum, though it can be seen in the large bowel and stomach. While little is known about its pathogenesis, gut microbiome disruption was associated with DFL in a case-control study. Disruption of the mucosal microbiota is also seen in nonalcoholic fatty liver disease (NAFLD).
Figure: Figure Legend: A) Endoscopic view of second portion of duodenum; B) CD21 stain identifying architecture of lymphoid follicles with positively staining dendritic reticulum cells; C) CD20 stain revealing lymphocytes within lymphoid follicles are overwhelmingly CD20-positive B cells; D) BCL-2 stain defines follicles as neoplastic and confirms diagnosis of follicular B-cell lymphoma.
Disclosures:
Thomas Checketts indicated no relevant financial relationships.
Manjushree Gautam indicated no relevant financial relationships.
Steven Mudrovich indicated no relevant financial relationships.
Thomas R. Checketts, DO1, Manjushree Gautam, MD2, Steven A. Mudrovich, MD3, Stevan A. Gonzalez, MD4. C0660 - Incidental Finding of a Duodenal-Type Follicular Lymphoma in NASH Cirrhosis: A Rare Malignancy With Favorable Outcomes, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.

.jpg "Thomas R. Checketts, DO photo")