University of Kansas Medical Center Kansas City, MO
Charlie Altfillisch, MD1, Pranay Reddy, MD, MPH2, Sachin Srinivasan, MD3, Mollie Jackson, DO4 1University of Kansas Medical Center, Kansas City, MO; 2Jefferson Health Northeast, Philadelphia, PA; 3University of Kansas Medical Center, Kansas City, KS; 4University of Kansas Health Systems, Kansas City, KS
Introduction: Gastrosplenic fistula (GSF) is a rare complication of diffuse large B cell lymphoma (DLBCL) involving the spleen or stomach. Fistulas can form spontaneously or following chemotherapy and occur due to local wall invasion. Presenting symptoms often include abdominal pain, splenomegaly, vomiting and fatigue. In this case we discuss a rare presentation of DLBCL complicated by GSF and abscess formation in a 36-year-old female presenting with abdominal pain with constipation.
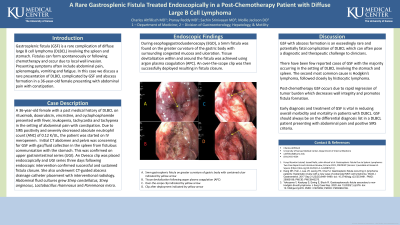
Case Description/Methods: A 36-year-old female with a past medical history of DLBCL on rituximab, doxorubicin, vincristine, and cyclophosphamide presented with fever, leukopenia, tachycardia and tachypnea in the setting of abdominal pain with constipation. Due to SIRS positivity and severely decreased absolute neutrophil count (ANC) of 0.12 K/UL, the patient was started on IV meropenem. Initial CT abdomen and pelvis was concerning for GSF with gas/fluid collection in the spleen from fistulous communication with the stomach. This was confirmed on upper gastrointestinal series (UGI). During esophagogastroduodenoscopy (EGD), a 5mm fistula was found on the greater curvature of the gastric body with surrounding congested mucosa and ulceration. Tissue devitalization within and around the fistula was achieved using argon plasma coagulation (APC). An over-the-scope clip was then successfully deployed resulting in fistula closure. Follow-up UGI three days later confirmed successful and sustained fistula closure. She also underwent CT-guided abscess drainage catheter placement with intervention radiology. Abdominal fluid cultures grew Step constellatus, Strep anginosus, Lactobacillus rhamnosus and Parvimonas micra.
Discussion: GSF with abscess formation is an exceedingly rare and potentially fatal complication of DLBCL which can often pose a diagnostic and therapeutic challenge to clinicians. There have been few reported cases of GSF with the majority occurring in the setting of DLCBL involving the stomach and spleen. The second most common cause is Hodgkin’s lymphoma, followed closely by histiocytic lymphoma. Post-chemotherapy GSF occurs due to rapid regression of tumor burden which decreases wall integrity and promotes fistula formation. Early diagnosis and treatment of GSF is vital in reducing overall morbidity and mortality in patients with DLBCL. GSF should always be on the differential diagnosis list in a DLBCL patient presented with abdominal pain and positive SIRS criteria.
Disclosures:
Charlie Altfillisch indicated no relevant financial relationships.
Pranay Reddy indicated no relevant financial relationships.
Sachin Srinivasan indicated no relevant financial relationships.
Mollie Jackson indicated no relevant financial relationships.
Charlie Altfillisch, MD1, Pranay Reddy, MD, MPH2, Sachin Srinivasan, MD3, Mollie Jackson, DO4. B0701 - A Rare Gastrosplenic Fistula Treated Endoscopically in a Post-Chemotherapy Patient With Diffuse Large B Cell Lymphoma, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.