Dina Alnabwani, MD1, Ankita Prasad, MD1, Prachi Patel, MBBS2, Priyaranjan Kata, MD3, Brian Wolfman, MD4, Pramil Cheriyath, MD, MS1 1Ocean University Medical Center, Brick, NJ; 2Holy Family University, Brick Township, NJ; 3Rutgers Health Community Medical Center, Toms River, NJ; 4Ocean University Medical Center, Brick Township, NJ
Introduction: Renal cell carcinoma (RCC) arises from renal tubular epithelial cells. Individuals with a family history of renal cancer have a twofold greater risk, indicating genetic factors. The triad of flank discomfort, hematuria, and flank mass is rare (10%) and indicates severe illness. 25% of patients had distant metastases or severe local-regional illness at the time of presentation. Lung, bones, liver, and brain are the most common sites of metastasis. Metastasis in the colon is rare, with very few documented cases. We present a case of post nephrectomy renal cell carcinoma with metastatic lesions in the intestine, peritoneum, and abdominal wall.
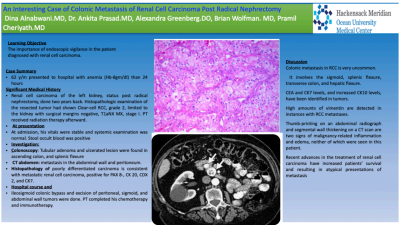
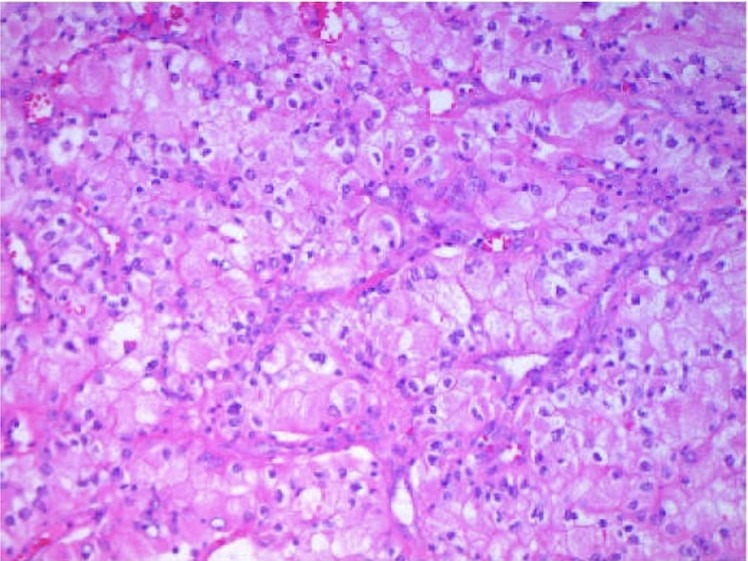
Case Description/Methods: A 62-year-old male presented with anemia with Hemoglobin of 8 gm/dl. He had a past medical history of renal cell carcinoma of the left kidney, status post radical nephrectomy, done 2 years ago. Histopathologic analysis of the excised tumor revealed grade 2 clear-cell RCC with negative surgical margins, T1aNxMx, stage I. Following that, he received radiation therapy. At admission, his vitals were stable and systemic examination was normal. Stool occult blood was positive. Tubular adenoma and ulcerated lesion were found in ascending colon and splenic flexure on colonoscopy. Computed Tomography (CT) scan of the abdomen showed the presence of tumor metastasis in the abdominal wall and peritoneum. Histopathology showed a poorly differentiated carcinoma consistent with metastatic renal cell carcinoma, positive for PAX 8-, CK 20, CDX 2, and CK7. He was treated with ileosigmoid colonic bypass and excision of peritoneal, sigmoid, and abdominal wall tumors. He later completed his chemotherapy and immunotherapy.
Discussion: Colonic metastasis in RCC is very uncommon. It can occur in the sigmoid, splenic flexure, transverse colon, and hepatic flexure. CEA and CK7 levels, and increased CK10 levels, have been identified in tumors. High amounts of vimentin are detected in instances with RCC metastases. Thumb-printing on an abdominal radiograph and segmental wall thickening on a CT scan are two signs of malignancy-related inflammation and edema, neither of which were seen in this patient. Recent advances in treating renal cell carcinoma have increased patient survival rates, leading to atypical presentations. This case report stresses the importance of endoscopic vigilance in patients diagnosed with renal cell carcinoma.
Dina Alnabwani indicated no relevant financial relationships.
Ankita Prasad indicated no relevant financial relationships.
Prachi Patel indicated no relevant financial relationships.
Priyaranjan Kata indicated no relevant financial relationships.
Brian Wolfman indicated no relevant financial relationships.
Pramil Cheriyath indicated no relevant financial relationships.
Dina Alnabwani, MD1, Ankita Prasad, MD1, Prachi Patel, MBBS2, Priyaranjan Kata, MD3, Brian Wolfman, MD4, Pramil Cheriyath, MD, MS1. B0129 - An Interesting Case of Anemia Related to Colonic Metastasis of Renal Cell Carcinoma Post Radical Nephrectomy, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.