St. Luke's University Health Network Bethlehem, PA
Brittney Shupp, DO, Janak Bahirwani, MD, Zarian Prenatt, DO, Hussam Tayel, MD, Gurshawn Singh, MD, Noel Martins, MD St. Luke's University Health Network, Bethlehem, PA
Introduction: Laparoscopic cholecystectomies (LC) have grown to become the gold standard treatment for symptomatic biliary disease, such as cholelithiasis. Each year, over 13 million LC are performed globally. Post Cholecystectomy Clip Migration (PCCM) is a known but rare complication of LC that occurs in less than 5% of cases. We present a case of PCCM presenting as choledocholithiasis that was successfully treated with Endoscopic Retrograde Cholangiopancreatography (ERCP).
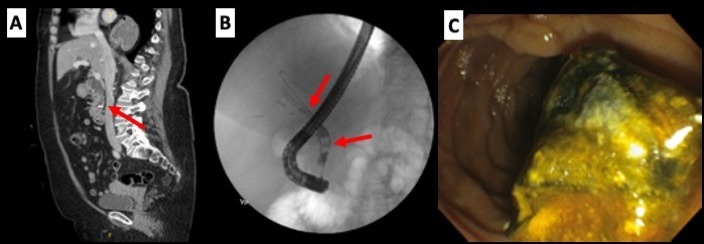
Case Description/Methods: A 68-year-old female with a history of laparoscopic cholecystectomy 7 years ago presented with the complaint of right lower quadrant abdominal pain and associated nausea with vomiting. On arrival, temperature was 97.6°, heart rate 86 beats per minute, and blood pressure 162/106 mmHg. Laboratory values were significant for an aspartate transaminase (AST) 192 U/L, alanine transaminase (ALT) 141 U/L, alkaline phosphatase 199 U/L, and total bilirubin 0.68 mg/dL. Follow up Computed Tomography (CT) abdomen/pelvis was completed and revealed a migrated cholecystectomy clip within the common bile duct (CBD) which measured 2.1 cm (Image 1A). Moderate intrahepatic biliary dilation was also noted. On the second day of admission, laboratory values peaked at AST 520 U/L, ALT 593 U/L, alkaline phosphatase 217 U/L, and total bilirubin 2.32 mg/dL. Patient was therefore taken for ERCP and guidewire canulation was completed without difficulty. Contrast was injected and the CBD was found to be dilated to a maximum diameter of 14 mm. Two floating filling defects were noted through use of fluoroscopy (Image 1B). One defect had a hyperdense focus suggesting the presence of the migrated clip. A major papilla sphincterotomy was performed, and two large stones were able to be successfully extracted. One of the two stones was found to have the migrated surgical clip embedded within it (Image 1C).
Discussion: During cholecystectomy, surgical clips are placed prior to transection of the cystic duct to allow for gallbladder removal. These clips remain in place for years without the need for removal but can act as a potential nidus for stone formation. Problems arise when the surgical clips migrate into the CBD, such as in this case, creating an obstructing pattern and requiring advanced intervention. Although rare, with the increasing number of LC being performed annually, the number of PCCM cases is expected to steadily rise making it imperative that physicians understand and recognize this potential complication.
Figure: Image 1: (A) CT abdomen/pelvis with contrast revealing a migrated cholecystectomy clip within the distal common bile duct which measured 2.1 cm. Moderate intrahepatic biliary dilation also noted. (B) ERCP with fluoroscopy demonstrating a floating filling defect due to stones in the distal and mid common bile duct. One clip noted to have a hyperdense focus consistent with migrated cholecystectomy clip. (C) Extraction of the stone with embedded cholecystectomy clip.
Disclosures:
Brittney Shupp indicated no relevant financial relationships.
Janak Bahirwani indicated no relevant financial relationships.
Zarian Prenatt indicated no relevant financial relationships.
Hussam Tayel indicated no relevant financial relationships.
Gurshawn Singh indicated no relevant financial relationships.
Noel Martins indicated no relevant financial relationships.
Brittney Shupp, DO, Janak Bahirwani, MD, Zarian Prenatt, DO, Hussam Tayel, MD, Gurshawn Singh, MD, Noel Martins, MD. D0027 - Now You See Me and Now You Don’t: A Rare Case of Post Cholecystectomy Clip Migration, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.