Richard Trieu, MD, Brandon Witten, BS, Aws Alameri, MD, Avin Aggarwal, MD University of Arizona, Tucson, AZ
Introduction: Portal cavernoma cholangiopathy (PCC) is defined as abnormalities in the biliary tree due to a portal cavernoma. Most cases occur in non-cirrhotic patients who remain asymptomatic. 5-30% of patients develop symptomatic disease and only 8% of symptomatic cases present with acute cholangitis. This case describes PCC as an uncommon cause of acute cholangitis.
Case Description/Methods: A 26-year-old male with a medical history of acute lymphocytic leukemia in remission, cryptogenic cirrhosis, and portal vein thrombosis (PVT) on warfarin presented with 2-weeks of worsening abdominal pain, darkening of the urine, and weight loss. On examination, he was febrile to 101°F, normotensive, and had both scleral and palatal icterus. Initial labs revealed white blood count: 13.5 x10(3)/mcL, total bilirubin 7.5mg/dL, & ALP 398U/L. MRCP showed biliary dilation related to extensive portal vein cavernous transformation and narrowing in the common bile duct (CBD) due to compression by cavernous vessels in porta hepatis. Endoscopic ultrasound (EUS) showed PVT and collateral flow. Endoscopic retrograde cholangiopancreatography (ERCP) revealed biliary narrowing and beading. These findings were diagnostic of cavernous transformation with cholangiopathy. The patient improved after biliary stent placement with repeat stenting 6 months later. There was a discussion about TIPS and Portal vein reconstruction. However, the patient did not follow through.
Discussion: PCC develops through PVT-related ischemia that underlies the development of collateral flow, biliary stricture, and dysmotility predisposing patients to cholangitis. Management is only indicated with symptomatic disease with endoscopic and surgical intervention. We report a rare presentation of PCC successfully managed with ERCP.
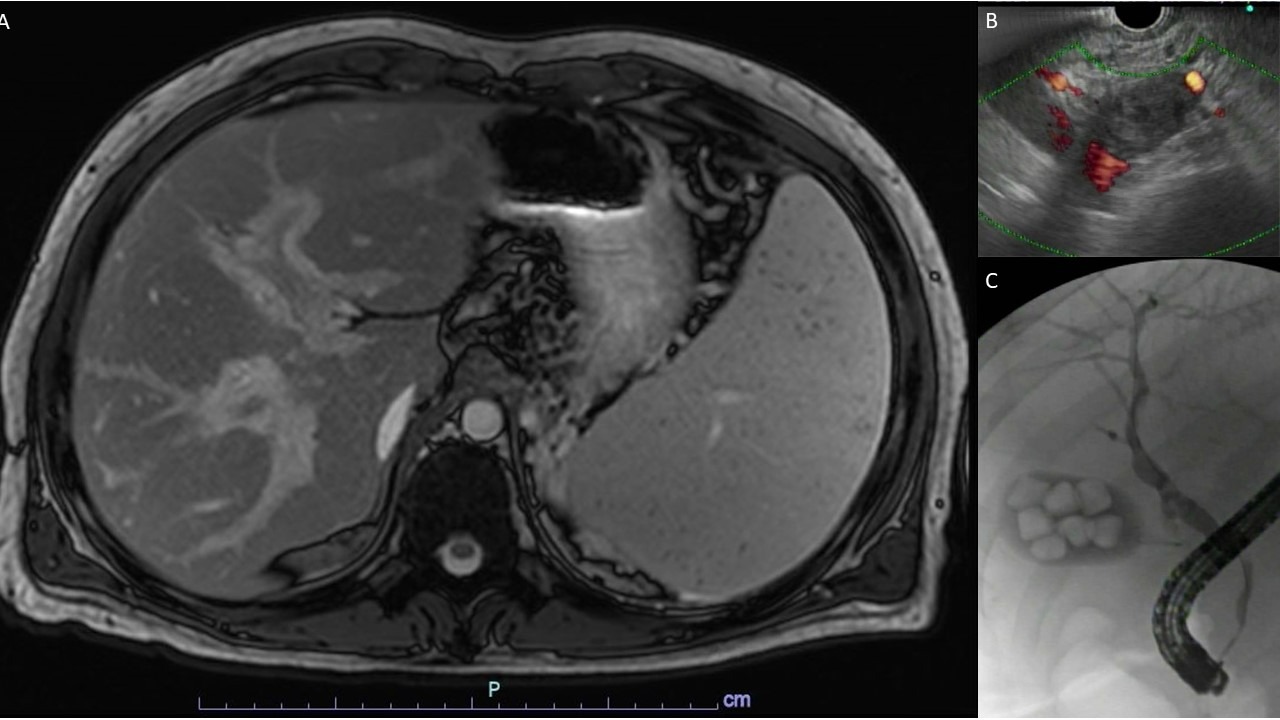
Figure: Figure 1: A) MRCP: Cavernous transformation of the portal vein. B) EUS: A portal vein thrombus involving area of portal vein confluence and collateral flow consistent with cavernous transformation. C) ERCP: Abnormal areas of narrowing and beading throughout the biliary system with extrinsic stenosis.
Disclosures:
Richard Trieu indicated no relevant financial relationships.
Brandon Witten indicated no relevant financial relationships.
Aws Alameri indicated no relevant financial relationships.
Avin Aggarwal indicated no relevant financial relationships.
Richard Trieu, MD, Brandon Witten, BS, Aws Alameri, MD, Avin Aggarwal, MD. D0032 - Portal Cavernoma Cholangiopathy Presenting With Acute Cholangitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.