Aaron Rampersad, MD1, Davis B. Berry, DO2, Luis Lizardo, MD1, Robert Farrar, MD1, Veeral Oza, MD3 1Prisma Health, Greenville, SC; 2East Tennessee State University, Johnson City, TN; 3University of South Carolina School of Medicine Greenville, Prisma Health, Greenville, SC
Introduction: The esophagus is a rare site for benign mucous duct cyst(mucocele). Mucoceles commonly occur from an obstructing salivary gland duct or rupture of the salivary gland. Therefore, mucoceles are most often found in the oral cavity. Symptomatic esophageal polyps or cysts have traditionally required surgical intervention. Endoscopic resection has become an option over the last few years and includes endoscopic mucosal resection or submucosal dissection. We present a case of an esophageal submucosal polypoid lesion that was removed endoscopically and revealed a rare and interesting pathology
Case Description/Methods: A 70 year old female was referred for evaluation of reflux symptoms. During her initial outpatient visit she described worsening reflux symptoms and dysphagia. initially having dysphagia just to liquids but now progressing to solids. A trial of pantoprazole significantly improved her reflux symptoms but her esophageal dysphagia persisted.
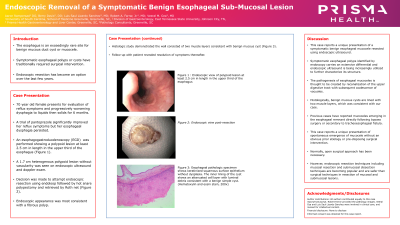
An upper endoscopy revealed a polypoid lesion at least 2.5 cm in length in the upper third of the esophagus (Figure 1a). A 2.5 cm heterogenous polypoid lesion without vascularity was seen on endoscopic ultrasound and doppler exam. Given lack of vascularity, the decision was made to attempt endoscopic resection. An endoloop was used to place at the base of the lesion, followed by resection(Figure 1b)
Endoscopic appearance was most consistent with a fibrous polyp. Histologic study demonstrated the wall consisted of two muscle layers consistent with benign mucous cyst (Figure 1c). On follow up patients’ symptoms had resolved
Discussion: A symptomatic esophageal polyp identified on an endoscopy carries an extensive differential diagnosis ranging from benign to malignant.
Esophageal mucoceles are thought to occur due to recanalization of the upper digestive tract with subsequent coalescence of vacuoles. Histologically, benign mucous cysts are lined with two muscle layers. Prior cases have reported mucoceles emerging in the esophageal remnant directly following bypass surgery or secondary to tracheoesophageal fistula. We report a unique case of spontaneous emergence of mucocele without an obvious prior etiology or pre-disposing surgical intervention.
Rarely, an esophageal cyst causes symptoms of dysphagia or regurgitation requiring removal. Endoscopic resection has gained popularity in recent years, due to the low rates of morbidity and mortality. Additional reports of esophageal mucoceles will help in understanding this rare condition better.
Figure: Fig 1a: Endoscopic appearance of an esophageal submucosal lesion; 1b: nodule post-resection ; 1c: Histologic study demonstrated the wall consisted of two muscle layers consistent with benign mucous cyst
Disclosures:
Aaron Rampersad indicated no relevant financial relationships.
Davis Berry indicated no relevant financial relationships.
Luis Lizardo indicated no relevant financial relationships.
Robert Farrar indicated no relevant financial relationships.
Veeral Oza: Boston Scientific – Consultant. S4 Medical – Advisor or Review Panel Member.
Aaron Rampersad, MD1, Davis B. Berry, DO2, Luis Lizardo, MD1, Robert Farrar, MD1, Veeral Oza, MD3. B0468 - Endoscopic Removal of a Symptomatic Benign Esophageal Sub-Mucosal Lesion, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.