D0042 - The Enigmatic Triangle of Hypertriglyceridemia-Induced Pancreatitis and Its Association With Diabetic Ketoacidosis and Resulting Pancreatic Pseudocyst: A Case Report
Garry Lachhar, MD, Elnaz Mahbub, DO, Cassidy Guida, DO, Andrew Melek, MS, Saloni Sachar, MS, Andrew Grees, MD, Sabrina Mohsin, DO, Alice Mei, DO, John Karstens, DO, Heidi Roppelt, MD, Nikolaos Hatzis, MD Stony Brook Southampton Hospital, Southampton, NY
Introduction: Acute pancreatitis (AP) presents with acute epigastric pain radiating to the back and elevated pancreatic enzymes. The most common causes are gallstones and alcohol. Hypertriglyceridemia-induced pancreatitis (HTGP), causes 14% of all AP cases, rising to 56% in pregnancy. We present a unique case of HTGP complicated by diabetic ketoacidosis (DKA) and pancreatic pseudocyst.
Case Description/Methods: A 27-year-old male with type 1 diabetes mellitus, hyperlipidemia, ADHD, and depression presented with sudden onset constant, sharp, diffuse abdominal pain with radiation to the back. He reported nausea, dry heaving, increased thirst and urinary frequency. Relevant family history includes familial hypertriglyceridemia. The patient was found to have DKA, lactic acidosis, leukocytosis, and hypocalcemia. Triglycerides (TG) and lipase/amylase were elevated. Computed tomography (CT) of the abdomen showed AP with fat stranding. He received fluids, an insulin drip, and was transferred to the intensive care unit. Patient met criteria for plasmapheresis and was transferred to a tertiary care center. On follow up, repeat CT three weeks post-presentation indicated a developing pseudocyst. CT four weeks later showed anterior pancreatic pseudocyst with a decrease of peripancreatic fluid collection and CT seven weeks later showed decreased peripancreatic and retroperitoneal fluid with 2 stents extending from stomach to collection.
Discussion: TG > 1000 is required for diagnosis of HTGP. TG 1000-1999 carries a 5% risk of developing HTGP, increasing to 20% in TG >2000. Patients are typically young, male, obese, and diabetic. AP may precipitate or complicate DKA. DKA can mask AP, occurring in approximately 10-15% of cases. In 100 consecutive cases of DKA, 11 had a CT confirmed AP with most caused by hypertriglyceridemia and alcohol. Hypocalcemia, lactic acidosis or sepsis necessitate intensive therapy including therapeutic plasma exchange (TPE), which replaces plasma with colloid solution. HTGP is managed with supportive care and insulin/TPE until TG < 500. TG< 200 prevents recurrence and is managed with pharmacotherapy and lifestyle modifications.
HTGP can cause AP and should be considered in the differential for acute abdominal pain, especially in younger males. It can be complicated by DKA and pancreatic pseudocyst, leading to a more severe presentation and necessitates the addition of TPE to insulin. Prompt recognition and management of HTGP is imperative in preventing complications and expediting recovery.
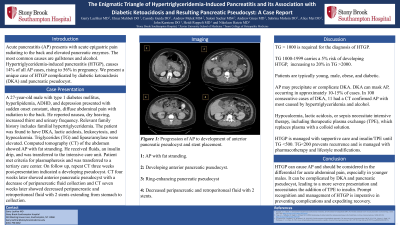
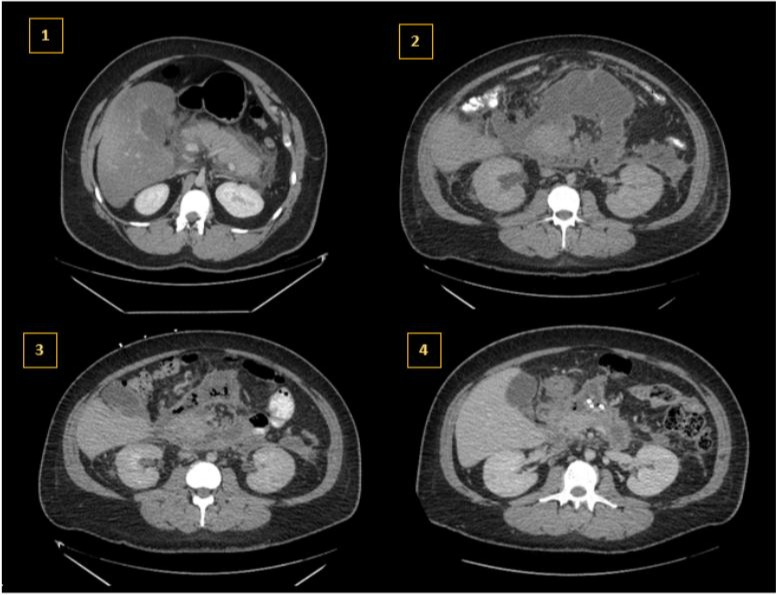
Figure: Progression of AP to development of anterior pancreatic pseudocyst and stent placement. 1: AP with fat stranding. 2: Developing anterior pancreatic pseudocyst. 3: Full development of pancreatic pseudocyst with ring enhancing. 4. Decreased peripancreatic and retroperitoneal fluid with 2 stents.
Disclosures:
Garry Lachhar indicated no relevant financial relationships.
Elnaz Mahbub indicated no relevant financial relationships.
Cassidy Guida indicated no relevant financial relationships.
Andrew Melek indicated no relevant financial relationships.
Saloni Sachar indicated no relevant financial relationships.
Andrew Grees indicated no relevant financial relationships.
Sabrina Mohsin indicated no relevant financial relationships.
Alice Mei indicated no relevant financial relationships.
John Karstens indicated no relevant financial relationships.
Heidi Roppelt indicated no relevant financial relationships.
Nikolaos Hatzis indicated no relevant financial relationships.
Garry Lachhar, MD, Elnaz Mahbub, DO, Cassidy Guida, DO, Andrew Melek, MS, Saloni Sachar, MS, Andrew Grees, MD, Sabrina Mohsin, DO, Alice Mei, DO, John Karstens, DO, Heidi Roppelt, MD, Nikolaos Hatzis, MD. D0042 - The Enigmatic Triangle of Hypertriglyceridemia-Induced Pancreatitis and Its Association With Diabetic Ketoacidosis and Resulting Pancreatic Pseudocyst: A Case Report, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.