Introduction: Syphilis is a rare cause of acute hepatitis. This report shows a case of syphilitic hepatitis mimicking Primary Biliary Cholangitis (PBC). This case shows syphilitic hepatitis presenting with an elevated alkaline phosphatase, and a positive Anti-Mitochondrial Antibody M2 subtype (AMA-M2). Treatment of the underlying syphilis with penicillin leads to resolution of the hepatitis and normalization of lab-work.
Case Description/Methods: A 53-year-old male was referred from his PCP for possible PBC.
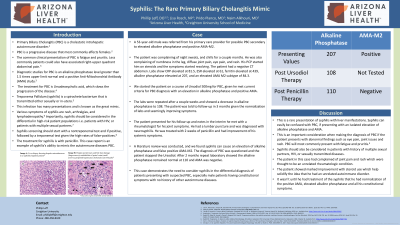
The patient was complaining of night sweats, and chills for a couple months. He was also complaining of diffuse joint pain, eye pain, and rash. He states his PCP started him on steroids which seemed to be resolving symptoms. The patient had A negative CT abdomen, CRP elevated at 81.5, ESR elevated at 61, ferritin elevated at 439, alkaline phosphatase elevated at 207, and had a positive AMA-M2 subtype count at 84.3.
We started the patient on a course of Ursodiol 500mg, since he met current criteria for PBC with an elevated alkaline phosphatase >1.5 times upper limit and a positive AMA. Repeat labs 4 weeks later showed alkaline phosphatase of 99.
Two months later the patient followed-up stating his rheumatologist did a lumbar puncture and found neurosyphilis. The patient was treated with penicillin and had improvement of symptoms. A literature review was conducted showing syphilis can cause an elevation of alkaline phosphatase and false positive AMA-M2. It was decided to stop Ursodiol for 2 months and repeat labs. Repeat laboratory showed alkaline phosphatase of 110 and negative AMA.
Discussion: A rare presentation of syphilis is with liver manifestations. Syphilis can easily be confused with PBC, with an isolated elevation of alkaline phosphatase, and AMA. This is an important consideration when making the diagnosis of PBC. Syphilis should be considered greater in patients with history of multiple sexual partners, patients with HIV, or other sexually transmitted diseases.
The patient in this case had complained of joint pain and rash which were thought to be an unrelated rheumatologic condition given improvement with steroids. Alkaline phosphatase was presumed to be artificially decreased secondary to the steroids before starting Ursodiol. Treatment of the underlying syphilis normalized lab values. This case demonstrates the need to consider syphilis in the differential diagnosis of patients presenting with suspected PBC, especially male patients with no history of other autoimmune diseases.
Disclosures:
Phillip Leff indicated no relevant financial relationships.
Lisa Rosch indicated no relevant financial relationships.
Prido Polanco indicated no relevant financial relationships.