William S. Reiche, DO, Faith Abodunrin, MD, Rajani Rangray, MBBS, Manasa Velagapudi, MBBS CHI Creighton University Medical Center, Omaha, NE
Introduction: Drug induced pancreatitis (DIP) is rare but potential cause of acute pancreatitis and accounts for 0.1-5.3% of all cases. In this case series, we report 2 cases of patients with doxycycline induced pancreatitis.
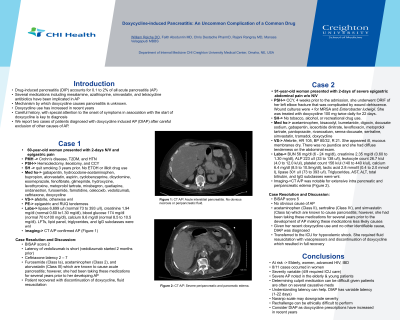
Case Description/Methods: A 60-year-old woman with cervical osteomyelitis on iv ceftriaxone and doxycycline presented with 2-day history of severe nausea, vomiting, and epigastric pain. On exam, she had epigastric and right upper quadrant tenderness. Laboratory evaluation was significant for serum lipase 6,699 u/l , creatinine of 1.94 mg/dl. Liver function tests and lipid panel were within normal limits. Computerized tomography (CT) of the abdomen and pelvis confirmed acute interstitial pancreatitis. Triglyceride, IgG subclasses and calcium levels were normal. Thorough review of her medications revealed doxycycline induced pancreatitis was suspected. Her symptoms gradually improved and lipase returned to 85 u/l with discontinuation of doxycycline.
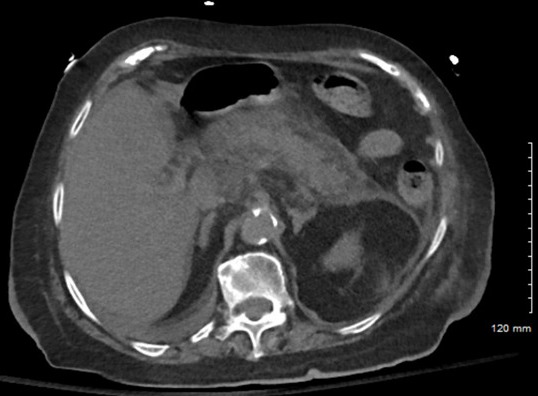
A 91year-old woman with recent history of left elbow fracture complicated by wound dehiscence on doxycycline therapy, presented for hospital admission with several days of increased confusion, malaise, and generalized, severe abdominal pain. She appeared ill, with dry mucous membranes and diffuse abdominal tenderness. Laboratory test results were notable for blood urea nitrogen (BUN) 56 mg/dl, creatinine 2.35 mg/dl, ALP 223 u/l, total bilirubin 1.1 mg/dl, wbc count 26.7 k/ul, calcium 6.4 mg/dl, lipase 301 u/l, AST, ALT, triglycerides and IgG subclass levels were within normal limits. CT abdomen showed extensive intrapancreatic and peripancreatic edema, the patient was diagnosed with severe pancreatitis. With careful exclusion of other etiologies, she was diagnosed with doxycycline induced pancreatitis. Her symptoms improved with aggressive hydration and discontinuation of doxycycline.
Discussion: Onset of symptoms with relation to starting the offending drug is key in identifying the causative agent of DIP. The severity, onset of symptoms, dosage of doxycycline and latency have been reported as variable as in our cases. Symptom onset was at 14 days of doxycycline therapy in the first vs 22 in the second case. Treatment includes cessation of doxycycline and aggressive IV fluid resuscitation. This case series emphasizes the importance of considering doxycycline as a cause of acute pancreatitis especially with its increased use in recent years.
Figure: Figure 1: CT abdomen with extensive intrapancreatic and peripancreatic edema (second case presented)
Disclosures:
William Reiche indicated no relevant financial relationships.
Faith Abodunrin indicated no relevant financial relationships.
Rajani Rangray indicated no relevant financial relationships.
Manasa Velagapudi indicated no relevant financial relationships.
William S. Reiche, DO, Faith Abodunrin, MD, Rajani Rangray, MBBS, Manasa Velagapudi, MBBS. D0053 - Doxycycline-Induced Pancreatitis: An Uncommon Complication of a Common Drug, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.