Walter Reed National Military Medical Center Bethesda, MD
Shane Mudrinich, MD1, Tudor Oroian, MD1, Sonja Dawsey, MD2 1Walter Reed National Military Medical Center, Bethesda, MD; 2Fort Belvoir Community Hospital, Fort Belvoir, VA
Introduction: Medullary carcinoma of the colon (MCC) represents < 3% of colon cancers and is characterized by microsatellite instability (MSI) leading to poor cellular differentiation. With its relative rarity and ambiguous histology, MCC remains a challenging, frequently-missed diagnosis.
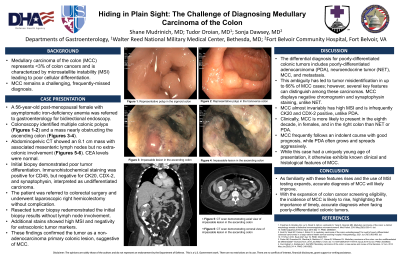
Case Description/Methods: A 56-year-old post-menopausal female with asymptomatic iron-deficiency anemia was referred to gastroenterology for bidirectional endoscopy. Colonoscopy identified multiple colonic polyps and a mass nearly obstructing the ascending colon. Abdominopelvic CT showed an 8.1 cm mass with associated mesenteric lymph nodes but no extracolonic involvement. CEA levels were normal. Initial biopsy demonstrated poor tumor differentiation. Immunohistochemical staining was positive for CD45, a marker of lymphocytic infiltration, but negative for cytokeratin (CK) 20, caudal-related homeobox gene 2 (CDX-2), and synaptophysin, interpreted as an undifferentiated carcinoma. The patient was referred to colorectal surgery and underwent laparoscopic right hemicolectomy without complication. Biopsy of the resected tumor redemonstrated the initial biopsy results without lymph node involvement. Additional stains showed high MSI and negativity for extracolonic tumor markers. These findings confirmed the tumor as a non-adenocarcinoma primary colonic lesion suggestive of MCC.
Discussion: The differential diagnosis for poorly-differentiated colonic tumors includes poorly-differentiated adenocarcinoma (PDA), neuroendocrine tumor (NET), MCC, and metastasis. This ambiguity has led to tumor misidentification in up to 66% of MCC cases; however, several key features can distinguish among these carcinomas. MCC displays negative chromogranin and synaptophysin staining, unlike NET. MCC almost invariably has high MSI and is infrequently CK20 and CDX-2 positive, unlike PDA. Clinically, MCC is more likely to present in the eighth decade, in females, and in the right colon than NET or PDA. MCC frequently follows an indolent course with good prognosis, while PDA often grows and spreads aggressively. While this case had a uniquely young age of presentation, it otherwise exhibits known clinical and histological features of MCC. As familiarity with these features rises and the use of MSI testing expands, accurate diagnosis of MCC will likely improve. With the expansion of colon cancer screening, the incidence of MCC is likely to rise, highlighting the importance of timely, accurate diagnosis when facing poorly-differentiated colonic tumors.
Disclosures:
Shane Mudrinich indicated no relevant financial relationships.
Tudor Oroian indicated no relevant financial relationships.
Sonja Dawsey indicated no relevant financial relationships.
Shane Mudrinich, MD1, Tudor Oroian, MD1, Sonja Dawsey, MD2. D0108 - Hiding in Plain Sight: The Challenge of Diagnosing Medullary Carcinoma of the Colon, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.