Sarah Grebennikov, DO1, David Y. Lo, MD, FACG2 1OhioHealth Riverside Methodist Hospital, Columbus, OH; 2Ohio Gastroenterology Group, Inc, and The Ohio State University College of Medicine, Columbus, OH
Introduction: Breast cancer is the second most common cancer in the US and the second leading cause of cancer related deaths. Breast cancer most commonly metastasizes to the bone, lung, liver, and brain, but rarely to the GI tract. We report a case of primary breast cancer with diffuse metastasis to the colon.
Case Description/Methods: 67-year-old female with history of collagenous colitis was diagnosed with stage lllA (T3, N2, M0) invasive lobular carcinoma (ILC) ER+/PR+/Her2+ of the left breast identified on screening mammogram. She initially underwent neoadjuvant chemotherapy and anti-HER-2/neu therapy followed by left modified radical mastectomy with lymph nodes positive for metastasis 8 months after initiating therapy. She also completed radiation to left chest wall. Two years later, she underwent prophylactic contralateral mastectomy with incidental finding of right breast cancer with unknown stage ER+/PR-/Her2-. Three years after diagnosis, she had a colonoscopy for early satiety and abdominal discomfort. Prior colonoscopy 2.5 years ago only showed diverticulosis, however this colonoscopy revealed diffuse congestion, erythema, induration, and ulceration (A) with stenotic ileocecal valve (B) concerning for inflammatory bowel disease (IBD). Multiple polyps were found in the cecum, descending, sigmoid and distal rectum. Forceps biopsies of all colonic segments and polypectomies demonstrated poorly differentiated adenocarcinoma (C). Staining matched breast cancer primary (ER+, PR-, HER2-; CK7 and GATA3+). CT showed abdominal lymphadenopathy and osteoblastic metastatic disease. Treatment was switched from Exemestane to Xeloda and Zometa was started for bone metastasis. At 15 months of follow up, she is tolerating therapy well with radiographic resolution of metastatic disease.
Discussion: Breast cancer rarely metastasizes to the GI tract (4.5%), the stomach being most commonly affected. Lobular subtype is more frequently implicated than ductular. Colonic involvement is rare and can mimic primary colon cancer and IBD. The latency period between initial diagnosis of breast cancer and discovery of colonic metastasis is variable and can occur up to 30 years after. Patients may present with bowel obstruction, or non-specific symptoms such as abdominal pain, diarrhea, and weight loss. This case illustrates that breast cancer metastasis to the colon can present with symptoms mimicking IBD and rarely causes secondary linitis plastica, which to our knowledge has never been reported involving the entire colon.
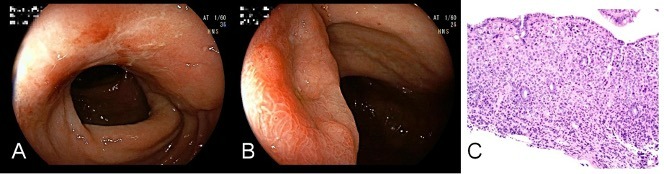
Figure: Colonoscopy with congestion, erythema, and ulceration (A). Stenotic ileocecal valve (B). Biopsy from entire colon, rectum, and polyps consistent with glandular mucosa infiltrated by poorly differentiated adenocarcinoma. Staining was positive for ER+, PR-, HER2-; additional staining was positive for CK7 and GATA3+ which is consistent with breast primary.
Disclosures:
Sarah Grebennikov indicated no relevant financial relationships.
David Lo indicated no relevant financial relationships.
Sarah Grebennikov, DO1, David Y. Lo, MD, FACG2. D0112 - Secondary Linitis Plastica of the Colon Due to Breast Cancer Metastasis Mimicking Inflammatory Bowel Disease, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.