Sneha Adidam, MD1, Naga Sai Shravan Turaga, MD2, Anish Konde, MD3 1Howard University Hospital, Washington, DC; 2University of Arkansas for Medical Sciences, Little Rock, AR; 3Providence Regional Cancer System, Lacey, WA
Introduction: Cancer of Unknown Primary (CUP) is defined as biopsy proven cancer thought to be metastatic in nature, without an identifiable primary site of origin, despite a thorough history and physical examination and standard imaging. We present an unusual case of squamous cell carcinoma (SCC) with unknown primary involving a retroperitoneal lymph node.
Case Description/Methods: A 55-year-old man with a history of hypertension, diabetes and left cerebral ischemic stroke presented with complaints of diffuse abdominal pain and constipation for 2 days. He had a weight loss of 30-40 pounds in 10 months. Initial vitals and labs were normal. Physical exam was significant for mild diffuse abdominal tenderness. Abdominal Computerized Tomography (CT) revealed diffuse retroperitoneal lymphadenopathy with a 1.5 cm celiac axis node with central attenuation suggestive of necrosis, a 2cm left periaortic lymph node. CT guided fine needle aspiration and core biopsy of right retrocaval lymph node was performed and histology revealed medium to large pleomorphic sheets of cells with surrounding large necrotic regions suggestive of moderate to poorly differentiated SCC. Immunohistochemical staining showed positive staining for p63 and CK 5/6 positive, negative staining for TTF1 and RCC. Skull base-mid thigh positron emission tomography (PET) CT revealed an area of hypermetabolic activity involving distal esophagus with standardized uptake value (SUV) of 6.3 and extensive retroperitoneal adenopathy with SUV of 4.5. Subsequently, given the high suspicion for esophageal primary, upper gastrointestinal endoscopy was done which showed a 38cm mass concerning for malignancy. Histological examination revealed moderately differentiated squamous cell carcinoma. He was started on chemoradiation for esophageal cancer.
Discussion: National Comprehensive Cancer Network guidelines discuss about workup for unknown primary with metastatic adenocarcinoma in retroperitoneal lymph nodes with but there is no description about workup for metastatic SCC. Furthermore, distal esophageal cancers are usually adenomatous in origin and metastasize to cervical lymph nodes. Hence, a thorough workup including PET-CT scan should be done in cases metastatic SCC involving retroperitoneal lymph nodes and distal esophageal SCC should be considered a differential in such cases.
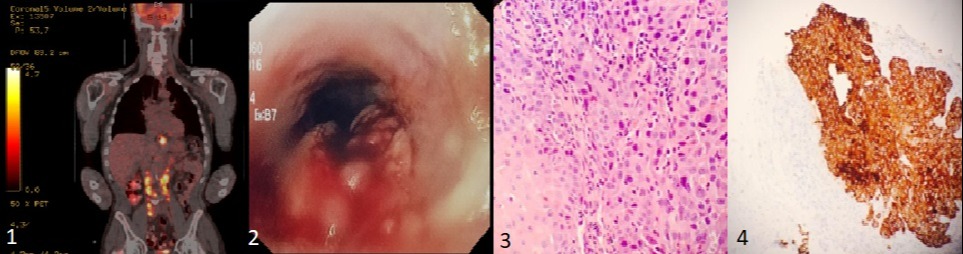
Figure: Image 1. shows skull base-mid thigh Positron Emission Technology CT scan which revealed an area of hypermetabolic activity involving distal esophagus with standard uptake value of 6.3. There was also extensive adenopathy peripancreatic, aortocaval space as well as periaortic space with FDG avid with SUV value of 4.5. Image 2. shows 38 cm mass in the mid-lower esophagus concerning for malignancy. Image 3. shows squamous cell carcinoma, invasive nests of squamous epithelial cells with moderate cytologic atypia. Image 4. shows immunostaining for cytokeratin shows diffuse positive staining supportive of squamous cell origin.
Disclosures:
Sneha Adidam indicated no relevant financial relationships.
Naga Sai Shravan Turaga indicated no relevant financial relationships.
Anish Konde indicated no relevant financial relationships.
Sneha Adidam, MD1, Naga Sai Shravan Turaga, MD2, Anish Konde, MD3. D0247 - The Conundrum of a Metastatic Retroperitoneal Lymph Node: Where Is the Primary Tumor?, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.