HCA/USF Morsani College of Medicine at HCA Florida Bayonet Point Hospital Hudson, FL
Glenn Garcia, MD1, Muhammed Hiba, MD2, Joseph Staffetti, MD1 1HCA/USF Morsani College of Medicine at HCA Florida Bayonet Point Hospital, Hudson, FL; 2HCA Florida Oak Hill Hospital, Brooksville, FL
Introduction: Russell Body Esophagitis (RBE) was first described in 2005 [1]. Diagnosis is made via identification of Russell Bodies (RBs) within plasma cells on biopsies of esophageal mucosa. RBs are cytoplasmic inclusions of immunoglobulins found in plasma cells. RBE is believed to share its pathogenesis with other gastrointestinal RBs. RBE is associated with Barrett’s Esophagus [1-4]. Russell Body Gastritis (RBG) [5] and Russell Body Duodenitis [6] have more published cases and an association with Helicobacter pylori [7].
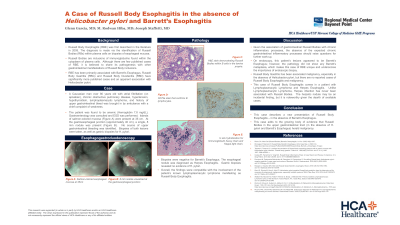
Case Description/Methods: An elderly man with lymphoplasmacytic lymphoma (LPL) presented with a chief complaint of weakness. The patient was found to be anemic, so Gastroenterology was consulted for further management. Esophagogastroduodenoscopy was performed. Islands of salmon-colored mucosa were present at 35 cm. At the GE junction (approximately 40 cm), an 8 mm nodule was present (Figure B). No source of upper gastrointestinal bleeding was identified. Biopsies were negative for Barrett’s Esophagus and H. pylori. The esophageal nodule was diagnosed as Herpes Esophagitis. H&E staining demonstrated pink globules within B Cells in the lamina propria (Figure C). The CD138 and CD79a stains confirmed the presence of lymphocytes. In situ hybridization for Kappa light chain showed clonal B lymphocytes. Additionally, clonal immunoglobulin heavy chain (IGH) and Kappa light chain (IGK) gene rearrangements were detected by PCR. Overall, the findings were compatible with RBE.
Discussion: The lesions appeared to be Barrett’s Esophagus; however, pathology did not show any Barrett’s metaplasia, making this case unique. RBG has been associated malignancy, especially in the absence of H. pylori, [8] but there are no reported cases of RBE and malignancy. LPL has been detected in the stomach and ileum; [9-11] LPL is classically known to cause the formation of RBs in bone marrow. [12] The presence of RBs in the esophagus is a possible manifestation of this patient’s LPL. This case adds to the growing body of evidence that RBs (in the absence of H. pylori and Barrett’s Esophagus) herald malignancy.
This case describes a new presentation of RBE – in the absence of Barrett’s Esophagus. Our case of RBE comes in a patient with LPL and Herpes Esophagitis. Unlike LPL, [10] Herpes infection has never been reported to be associated with RBs in the gastrointestinal tract. The herpetic nodule are noteworthy given herpesviruses are a known source of Russell Body Cervicitis. [13]
Figure: Figure A (Left): Salmon-colored mucosa visualized at 35cm. Figure B (right): 8 mm herpetic nodule observed at gastroesophageal junction.
Disclosures:
Glenn Garcia indicated no relevant financial relationships.
Muhammed Hiba indicated no relevant financial relationships.
Joseph Staffetti indicated no relevant financial relationships.
Glenn Garcia, MD1, Muhammed Hiba, MD2, Joseph Staffetti, MD1. A0211 - Russell Body Esophagitis: A Possible Indication to Screen for Hematologic Malignancy, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.