Maria Gabriela Rubianes Guerrero, MD, Donald P. Kotler, MD Jacobi Medical Center, Bronx, NY
Introduction: Before the era of biologic agents, corticosteroids were the most effective therapy available for inflammatory bowel disease (IBD) as well as other inflammatory and immune-mediated disorders, and treatment often was prolonged. As a result, many patients developed secondary adrenal insufficiency, in which the normal circadian rhythm of cortisol secretion was maintained but a defect in the cortisol response to stress persisted, as was the risk of adrenal crisis in response to severe physiologic stress. As corticosteroids are no longer used chronically in IBD, adrenal crisis has become a rare complication, and many gastroenterologists have no personal experience with it. We recently saw such a case which we are presenting as a reminder of its continued existence.
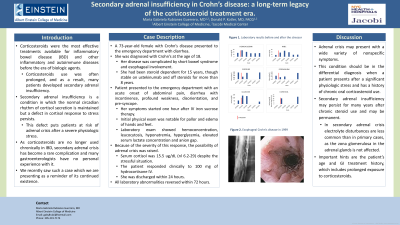
Case Description/Methods: A 73-year-old female with Crohn’s disease diagnosed at the age of 18, complicated by short bowel syndrome and esophageal involvement, who had been steroid dependent for 15 years though stable on ustekinumab and no steroids for more than 8 years, presented to the emergency department with an acute onset of abdominal pain, diarrhea with incontinence, profound weakness, disorientation, and possible syncope, one hour after IV iron sucrose therapy. Initial physical exam was notable for pallor and edema of hands and feet. Laboratory exams showed hemoconcentration, leukocytosis, hyponatremia, plus elevated serum lactate concentration and anion gap. Because of the severity of this response, the possibility of adrenal crisis was raised: serum cortisol was 15.5 ug/dL (nl 6.2-29) despite the stressful situation and the patient responded clinically to 100 mg of hydrocortisone IV. She was discharged within 24 hours and all laboratory abnormalities reversed within 72 hours.
Discussion: Adrenal crisis can present with a wide variety of nonspecific symptoms and should be in the differential diagnosis when a patient presents after a significant physiologic stress and has a history of chronic oral corticosteroid use. Electrolyte disturbances are less common in secondary adrenal insufficiency as the zona glomerulosa of the adrenal gland is not affected. Secondary adrenal insufficiency may persist for many years after chronic steroid use and may be permanent. In patients with secondary adrenal insufficiency. Important hints are the patient’s age and GI history, which includes extent of exposure to corticosteroids. Effective diagnosis requires maintaining a high index of suspicion.
Disclosures:
Maria Gabriela Rubianes Guerrero indicated no relevant financial relationships.
Donald Kotler indicated no relevant financial relationships.
Maria Gabriela Rubianes Guerrero, MD, Donald P. Kotler, MD. C0439 - Adrenal Crisis in a Patient With Crohn’s Disease: A Legacy of the Corticosteroid Treatment Era, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.