Fnu Deepali, MBBS, Prabh G. Singh, MBBS, Michal Reid, MD, Louis Wong Kee Song, MD, Navtej Buttar, MD Mayo Clinic, Rochester, MN
Introduction: Complications such as esophago-bronchial/pleural fistulas are the source of considerable morbidity/mortality. Surgical management is not possible in all patients and recurrence after conventional methods like clipping is common. Our aim was to develop novel endoscopic strategies to treat these fistulas where conventional methods either failed or were not advised.
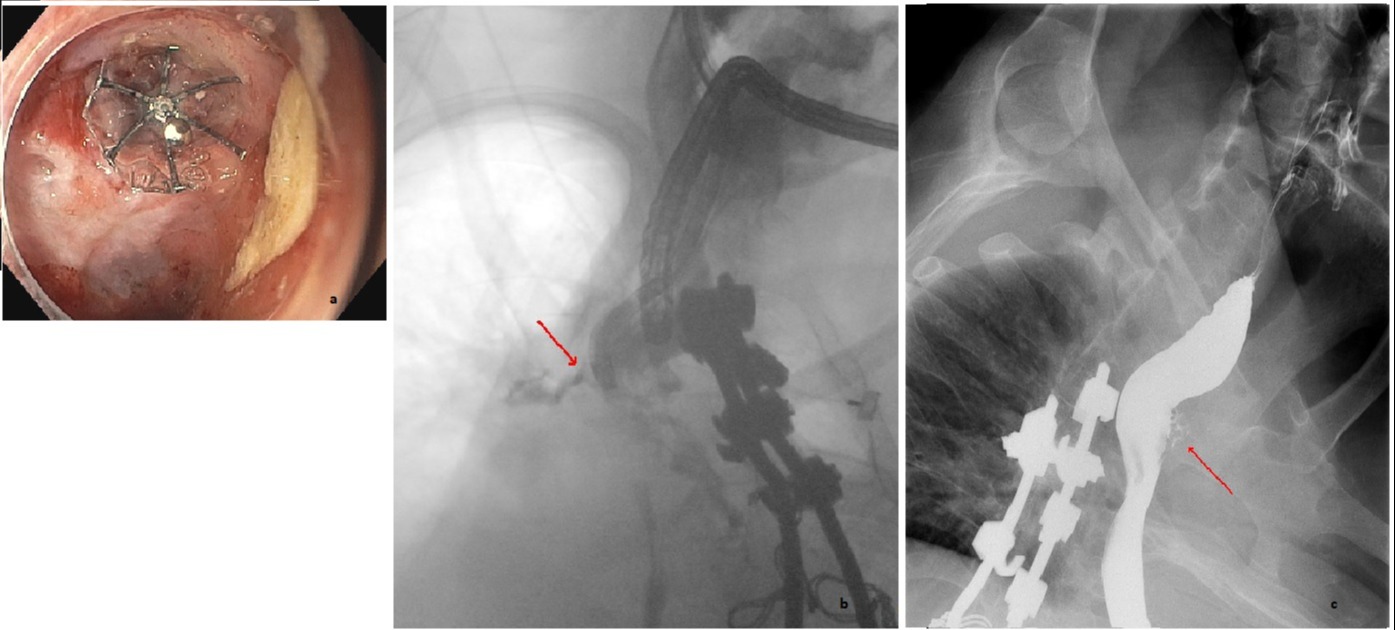
Case Description/Methods: We used a combined endoscopic bronchoscopic approach to place a spiration valve in the management of non-healing, recurrent esophago-bronchial/pleural fistulas. A case report presented here illustrates this concept- in January 2022, a 39-year-old male with an esophago-bronchial fistula was treated with placement of a spiration valve. He was diagnosed in 2020, when he presented with an esophageal diverticulum with a fistulous opening at the base of the diverticula (Fig 1b). This was treated with a padlock clip which subsequently migrated. A repeat padlock clip was placed which migrated again with the formation of exuberant granulation tissue likely related to the padlock clip. Considerable edema was noted, and a feeding tube was placed so that edema could resolve before deciding about further intervention. A decision was made to use a combined endoscopic bronchoscopic approach to place a spiration valve. Valve placement was challenging, and a 9 mm valve was used (Fig 1a). It was accomplished under fluoroscopic, endoscopic and bronchoscopic guidance. Only a small amount of contrast leak was noted and that too only when contrast was injected under pressure in the esophagus.
Discussion: Immediate clinical success was noted. Fluoroscopic esophagogram after 14 days showed no oral contrast entering the tracheobronchial tree. Further follow up esophagograms in February and March 2022 showed persistent but considerably improved sinus tract adjacent to the spiration valve (Fig 1c).
Conclusion: Spiration valve placement is an effective way to manage esophago-bronchial/pleural fistulas especially where conventional methods have either failed or were not feasible. Trials on more cases are required to see the efficacy of this novel approach.
Figure: a- Spiration Valve in place (endoscopic image) b- TEF before treatment (fluoroscopic image) c- Spiration valve in situ controlling the leak (fluoroscopic image)
Disclosures:
Fnu Deepali indicated no relevant financial relationships.
Prabh Singh indicated no relevant financial relationships.
Michal Reid indicated no relevant financial relationships.
Louis Wong Kee Song: Intuitive Surgical – Consultant. Intuitive Surgical, Inc. – Consultant. Steris – Consultant. Steris Inc. – Consultant.
Navtej Buttar indicated no relevant financial relationships.
Fnu Deepali, MBBS, Prabh G. Singh, MBBS, Michal Reid, MD, Louis Wong Kee Song, MD, Navtej Buttar, MD. C0482 - Spiration Valve to Manage Esophago-Bronchial/Pleural Fistulas: A Novel Approach, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.