Tim Brotherton, MD1, Laith Numan, MD1, Samer Al-Kaade, MD2 1Saint Louis University, St. Louis, MO; 2Mercy Clinic Gastroenterology, St. Louis, MO
Introduction: Aortoesophageal fistula is a devastating cause of upper gastrointestinal bleeding that occurs due to pathologic communication of the esophagus with the aorta. Risk factors include thoracic aortic aneurysm, foreign body ingestion, esophageal cancer, post-surgical complications, and prior radiation therapy. We describe a case of a patient who developed hemorrhaging into the esophagus due to aortoesophageal fistula during esophagogastroduodenoscopy (EGD).
Case Description/Methods: Our patient is a 52-year-old man presenting with hematemesis and hematochezia. He has history of non-small cell lung cancer treated with chemoradiation. Treatment has been complicated by esophageal strictures that have required dilation. On EGD, he was noted to have a visible vessel at the site of a scar in the mid esophagus where he had previously had stricture. Initially, no bleeding was visualized. However, during the exam, the patient developed coughing and began to have profuse bleeding in the mid esophagus. Bleeding was uncontrolled despite epinephrine injection, thermal therapy with gold probe, hemostatic clip, and hemospray. Two fully covered esophageal stents were placed but were unsuccessful in tamponading the area. An esophageal dilation balloon was insufflated within the stents for temporary control.
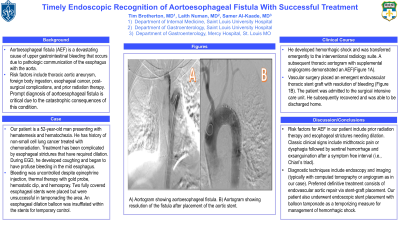
He developed hemorrhagic shock and was transferred emergently to the interventional radiology suite. A subsequent thoracic aortogram with supplemental angiograms demonstrated an aortoesophageal fistula (Figure 1A). Vascular surgery placed an emergent endovascular thoracic stent graft with resolution of bleeding (Figure 1B). The patient was admitted to the surgical intensive care unit. He subsequently recovered and was able to be discharged home.
Discussion: Prompt diagnosis of aortoesophageal fistula is critical due to the catastrophic consequences of this condition. Risk factors present in our patient include prior radiation therapy and esophageal strictures needing dilation. Classic clinical signs include midthoracic pain or dysphagia followed by sentinel hemorrhage and exsanguination after a symptom free interval (i.e., Chiari’s triad). Other diagnostic techniques include endoscopy and imaging (typically with computed tomography or angiogram as in our case). Preferred definitive treatment consists of endovascular aortic repair via stent-graft placement. Our patient also underwent endoscopic stent placement with balloon tamponade as a temporizing measure for management of hemorrhagic shock.
Figure: A) Aortogram showing aortoesophageal fistula. B) Aortogram showing resolution of the fistula after placement of the aortic stent.
Disclosures:
Tim Brotherton indicated no relevant financial relationships.
Laith Numan indicated no relevant financial relationships.
Samer Al-Kaade: AbbVie – Advisory Committee/Board Member. Abbvie – Speakers Bureau. Aimmune Therapeutics, a Nestlé Health Science company – Consultant, Medical Writing Support. HYDE, Love&Overby, LLP – Consultant.
Tim Brotherton, MD1, Laith Numan, MD1, Samer Al-Kaade, MD2. D0340 - Timely Endoscopic Recognition of Aortoesophageal Fistula With Successful Treatment, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.