East Tennessee State University Johnson City, Tennessee
Fitsum Woldesellassie, MD1, Andres R. Diaz, MD1, Mark Young, MD1, Samantha Grant, MD2 1East Tennessee State University, Johnson City, TN; 2Northeast Georgia Medical Center, Gainesville, GA
Introduction: Adenocarcinoma of small the bowel is a rare entity with less than 3% of gastrointestinal cancers. The duodenum is the most involved segment of the small bowel followed by the jejunum and ileum. Duodenal bulb adenocarcinoma is, however, an extremely rare finding with very few cases reported. In this case, we present primary duodenal bulb adenocarcinoma that manifested as epigastric pain with nausea.
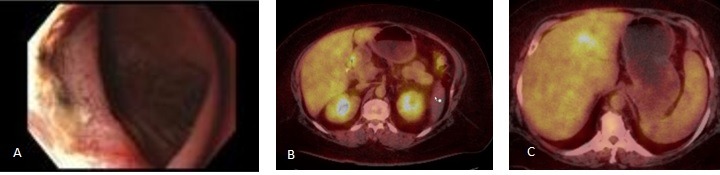
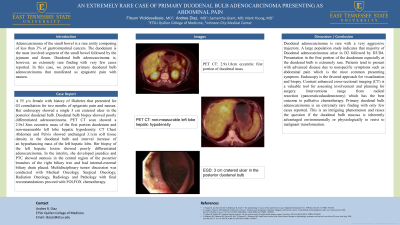
Case Description/Methods: 55 y/o female with history of Diabetes that presented for GI consultation for two months of epigastric pain and nausea. Her endoscopy showed a single 3 cm cratered ulcer in the posterior duodenal bulb. Duodenal bulb biopsy showed poorly differentiated adenocarcinoma. PET CT scan showed a 2.9x1.8cm eccentric mass of the first portion duodenum and non-measurable left lobe hepatic hypodensity. CT Chest Abdomen and Pelvis showed unchanged 3.1cm soft tissue density in the duodenal bulb and interval increase of an hypoehancing mass of the left hepatic lobe. Her biopsy of the left hepatic lesion showed poorly differentiated adenocarcinoma. In the interim, she developed jaundice and PTC showed stenosis in the central region of the posterior branches of the right biliary tree and had internal-external biliary drain placed. Multidisciplinary tumor discussion was conducted with Medical Oncology, Surgical Oncology, Radiation Oncology, Radiology and Pathology with final recommendations proceed with FOLFOX chemotherapy.
Discussion: Duodenal adenocarcinoma is rare with a very aggressive trajectory. A large population study indicates that majority of Duodenal adenocarcinoma arise in the D2 followed by D3/D4. Presentation in the first portion of the duodenum especially at the duodenal bulb is extremely rare. Patients tend to present with advanced disease due to nonspecific symptoms such as abdominal pain which is the most common presenting symptom. Endoscopy is the favored approach for visualization and biopsy. Contrast enhanced cross-sectional imaging (CT) is a valuable tool for assessing involvement and planning for surgery. Interventions ranges from radical resection (pancreaticoduodenectomy) which has the best outcome to palliative chemotherapy. Primary duodenal bulb adenocarcinoma is an extremely rare finding with only few cases reported. This is an intriguing phenomenon and raises the question if the duodenal bulb mucosa is inherently advantaged environmentally or physiologically to resist to malignant transformation.
Figure: Figure A: Endoscopic imaging finding of 3 cm cratered ulcer in the posterior duodenal bulb Figure B: PET CT scan showing 2.9x1.8cm eccentric mass of the first portion duodenum Figure C: PET CT scan showing non-measurable left lobe hepatic hypodensity
Disclosures:
Fitsum Woldesellassie indicated no relevant financial relationships.
Andres Diaz indicated no relevant financial relationships.
Mark Young indicated no relevant financial relationships.
Samantha Grant indicated no relevant financial relationships.
Fitsum Woldesellassie, MD1, Andres R. Diaz, MD1, Mark Young, MD1, Samantha Grant, MD2. A0646 - An Extremely Rare Case of Primary Duodenal Bulb Adenocarcinoma Presenting as Epigastric Abdominal Pain, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.

.jpg "Fitsum Woldesellassie, MD photo")