Ian M. Greenberg, MD, David S. Braun, MD, Prashant Kedia, MD Methodist Dallas Medical Center, Dallas, TX
Introduction: “Candy cane” syndrome is a post-surgical Roux-en-Y gastric bypass (RYGB) complication associated with a markedly long, surgically-created blind end of the afferent Roux limb distal to the gastrojejunostomy. Gradual filling of this long blind limb with food can result in symptoms, including postprandial epigastric pain, nausea, vomiting, or regurgitation. Treatment of candy cane syndrome traditionally consists of laparoscopic resection of the redundant blind afferent limb. We present the first case of successful treatment of candy cane syndrome through endoscopic revision of the gastrojejunal (GJ) anastomosis.
Case Description/Methods: A 40-year-old female presented for evaluation of intractable acid reflux, nausea, and weight recidivism eight years post RYGB. Esophagogastroduodenoscopy revealed evidence of prior RYGB, a healthy-appearing GJ anastomosis, a direct path across the GJ anastomosis into the blind afferent limb, and the enteral efferent limb located at a more angulated orientation toward the 4:00 position. An upper gastrointestinal series revealed an exaggerated blind afferent limb with pooling of contrast in the afferent blind limb before spilling to progress down the Roux limb. This finding suggested the reflux likely stemmed from the excessively long blind afferent limb. The patient wished to avoid surgery and a novel endoscopic suturing technique was performed that narrowed the GJ anastomosis and oriented flow towards the enteral efferent limb. This resulted in 1) limiting acid reflux 2) assisting with weight loss and 3) redirecting flow of contents more toward the enteral efferent limb. Post-procedure our patient had no additional weight gain and her acid reflux and nausea resolved.
Discussion: Candy cane syndrome is an underappreciated complication reported following RYGB. It results from an excessively long blind afferent Roux limb at the gastrojejunostomy that can lead to food accumulation. Patients often present with nausea, vomiting, food intolerance, acid reflux, and abdominal pain. Many patients remain undiagnosed due to vague gastrointestinal symptoms, delayed presentation, and physician unawareness. Historically, treatment has required surgical revision. Endoscopic suturing revision of the GJ anastomosis can provide an alternative less invasive and possibly safer treatment option that address the reflux symptoms, weight regain, and aberrant flow of contents into the blind limb.
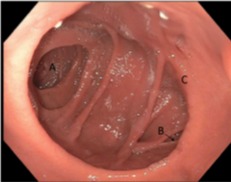
Figure: Fig. 1: Endoscopic view of direct access into the blind afferent limb A, the acute angle of the enteral efferent limb B, and dilated gastrojejunal anastomosis C.
Disclosures:
Ian Greenberg indicated no relevant financial relationships.
David Braun indicated no relevant financial relationships.
Prashant Kedia indicated no relevant financial relationships.
Ian M. Greenberg, MD, David S. Braun, MD, Prashant Kedia, MD. D0455 - Successful Treatment of “Candy Cane” Syndrome Through Endoscopic Gastrojejunal Anastomosis Revision, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.