Vikash Kumar, MD1, Aditya Chauhan, MD1, Praneeth Bandaru, MD1, Vijay Gayam, MD1, Jasparit Minhas, MD1, Lubna Attal, MD1, Dhir Gala, BS2, Salman Haider, MD1, Rewanth Katamreddy, MD3, Derrick Cheung, MD1 1The Brooklyn Hospital Center, Brooklyn, NY; 2American University of the Caribbean School of Medicine, Brooklyn, NY; 3Saint Michael's Medical Center, Newark, NJ
Introduction: Non-islet cell tumor hypoglycemia (NICTH) is a rare paraneoplastic syndrome that leads to the release of insulin-like growth factor-2 (IGF-2). It is commonly associated with tumors of mesenchymal origin like gastrointestinal stromal tumors (GIST).
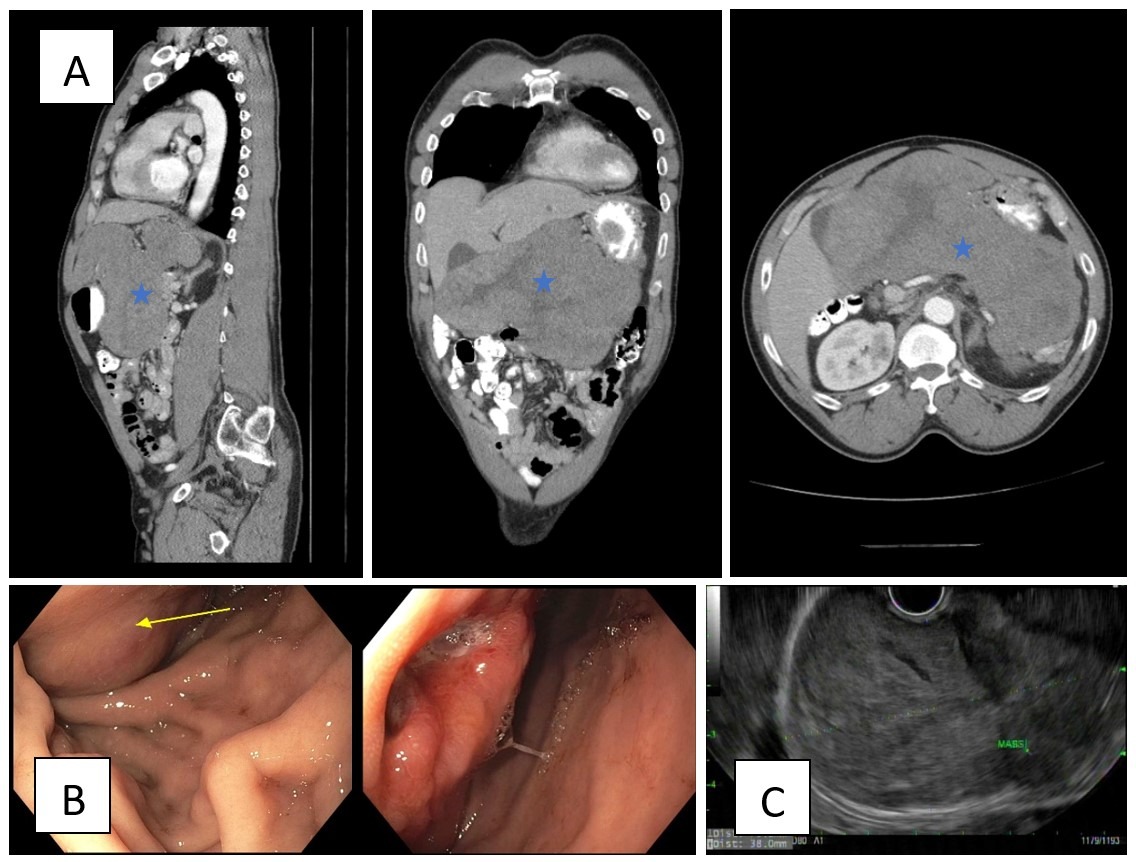
Case Description/Methods: A 62-year-old male, with a past medical history of recently diagnosed GIST was started on imatinib but stopped taking it one month ago pending surgical evaluation, presents with altered mental status due to severe hypoglycemia. The patient had no prior history of diabetes or adrenal insufficiency. The patient's repetitive finger sticks glucose remained persistently low even after good oral intake and two D50 pushes. Urine toxicology and drug screen for sulfonylureas were negative. Laboratory investigations showed reduced levels of insulin, C-peptide, and insulin-like growth factor-1 (IGF-1), but his IGF-2 was increased. Endocrinology was consulted for refractory hypoglycemia; recommended to start D10 fluids in the setting of resistant low blood glucose and start octreotide and steroids. Insulinoma was unlikely as insulin and C-peptides were low. CT chest/abdomen/pelvis shows grossly unchanged gastric GIST, measuring 25 x 19.6 x 11.4 cm with no evidence of metastatic disease in the abdomen or pelvis (Figure 1A). Esophagogastroduodenoscopy (EGD) demonstrated large, bilobed subepithelial mass measuring 10-15 cm with an area of ulceration within the mass (Figure 1B) followed up with Endoscopic ultrasound (EUS) demonstrating subepithelial lesion was found likely arising from the fundus, lesser curve and body of the stomach, layer of origin could not be determined on due to the large size of the mass (Figure 1C). Oncology was consulted for further management of malignancy; imatinib was resumed and referred for surgical evaluation for tumor removal.
Discussion: IGF-II acts as an autocrine growth factor in tumor cells therefore, it is highly likely that IGF-II will be high in case of high tumor bulk and making them at high risk of developing NICTH. In patients diagnosed with GIST with hypoglycemic symptoms, we should consider IGF-II secreting GIST in addition to insulinoma especially in bulky tumors.
Figure: Figure 1A: CT scan abdomen/pelvis with contrast showing large soft tissue density mass inseparable from the lesser curvature of the stomach marked with asterisk. Figure 1B: EGD findings consistent with a large, bilobed subepithelial mass measuring 10-15 cm with an area of ulceration within the mass (seen best on retroflexion) was found on the lesser curvature of the stomach along the anterior wall of the stomach. Figure 1C: Endoscopic US findings showed A 43.0 mm x 77.8 mm subepithelial lesion was found likely arising from the fundus, lesser curve and body of the stomach s/p FNB x 4. The lesion was hypoechoic and had some cystic spaces within it in some areas. Sonographically, the lesion appeared to originate from the stomach, but the wall layers could not be determined due to the large size of the mass.
Disclosures:
Vikash Kumar indicated no relevant financial relationships.
Aditya Chauhan indicated no relevant financial relationships.
Praneeth Bandaru indicated no relevant financial relationships.
Vijay Gayam indicated no relevant financial relationships.
Jasparit Minhas indicated no relevant financial relationships.
Lubna Attal indicated no relevant financial relationships.
Dhir Gala indicated no relevant financial relationships.
Salman Haider indicated no relevant financial relationships.
Rewanth Katamreddy indicated no relevant financial relationships.
Derrick Cheung indicated no relevant financial relationships.