Loma Linda University Medical Center Loma Linda, CA
Masuma Syed, MD, Xin Zheng, DO, Mina Rakoski, MD Loma Linda University Medical Center, Loma Linda, CA
Introduction: The etiology of liver disease in pregnancy can be challenging to diagnose as it may be related to the pregnancy or completely independent. Several disorders can cause elevated LFTs during pregnancy including the syndrome of hemolysis, elevated liver tests, and low platelets (HELLP) and acute fatty liver of pregnancy (AFL). There is often difficulty differentiating between HELLP and AFL, both of which are life-threatening complications of pregnancy. This vignette is an example of the complexity involved in differentiating between these pregnancy-associated liver diseases.
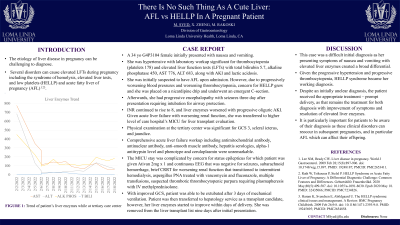
Case Description/Methods: A 34 yo G4P3104 female initially presented with nausea and vomiting. She was hypertensive with laboratory workup significant for elevated LFTs with total bilirubin 5.7, ALP 450, AST 776, ALT 683, along with AKI. She was initially suspected to have AFL at admission, however due to progressively worsening blood pressures and development of thrombocytopenia (platelets 13), HELLP syndrome was suspected so she was placed on a nicardipine drip and underwent an emergent C-section. Liver and renal function continued to decline postpartum so patient briefly required CRRT with eventual transition to HD. Due to rising INR and LFTs in the setting of worsened lethargy, she was diagnosed with acute liver failure and urgently listed for liver transplant status 1a. Comprehensive acute liver failure workup included negative AMA, ANA, ASMA, hepatitis serologies, alpha-1 antitrypsin level and phenotype and ceruloplasmin. After requiring mechanical ventilation for several days, patient was extubated due to improved GCS and transferred out of ICU. She remained listed for liver transplant, however, her LFTs started to improve within days of delivery. She was removed from the liver transplant list nine days after presentation.
Discussion: This case was a difficult diagnosis as her presenting symptoms of nausea and vomiting with elevated LFTs created a broad differential. Given the progressive hypertension and thrombocytopenia, she was diagnosed with HELLP syndrome. Despite an initially unclear diagnosis, the patient received the appropriate treatment – prompt delivery, as that remains the treatment for both diagnoses. After an initial decline in liver and kidney function immediately postpartum, symptoms rapidly improved with full resolution of elevated liver enzymes and coagulopathy. It is particularly important for patients to be aware of their diagnosis as these clinical disorders can reoccur in subsequent pregnancies.
Disclosures:
Masuma Syed indicated no relevant financial relationships.
Xin Zheng indicated no relevant financial relationships.
Mina Rakoski indicated no relevant financial relationships.
Masuma Syed, MD, Xin Zheng, DO, Mina Rakoski, MD. D0566 - There Is No Such Thing as a Cute Liver: AFL vs HELLP in a Pregnant Patient, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.