Alex Blachowicz, MD, Steven Hendler, MD, Marcel Ghanim, MD Loyola University Medical Center, Maywood, IL
Introduction: Hepatocellular Carcinoma (HCC) is a potential complication of cirrhosis. Liver transplantation is often viewed as curative of HCC when fulfilling the Milan criteria prior to surgery. However, recurrence rates of HCC post-transplant remain high. Here, we present a case of post-transplant HCC recurrence presenting as a bleeding gastric ulcer.
Case Description/Methods: A 72-year-old Caucasian female presented with coffee-ground emesis. Three years prior, she had orthotopic liver transplantation due to hepatitis C virus (HCV) related cirrhosis, previously treated with Vosevi/ribavarin with sustained virologic response and HCC with evidence of moderate differentiation and focus of vascular invasion on explanted liver.
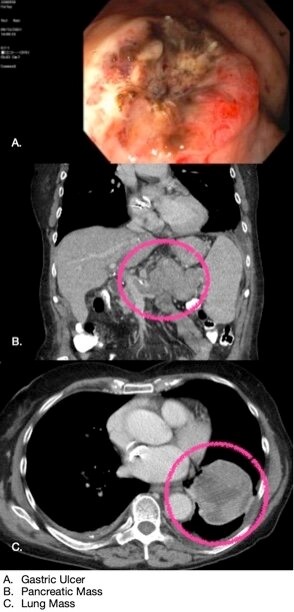
Upper endoscopy revealed a cratered gastric ulcer with heaped edges. Biopsies from the ulcer edges showed poorly differentiated adenocarcinoma with signet ring features. Immunohistochemical testing showed tumor cells positive for CK8/18, Glutamine Synthetase, and polyclonal CEA with canalicular pattern; features consistent with high grade HCC.
CT scan revealed a necrotic mass replacing most of the pancreatic body and tail, a lung mass and multiple vertebral compression fractures. Fine needle biopsy of pancreatic mass was consistent with metastatic carcinoma compatible with HCC.
Discussion: Tumor recurrence post-liver transplantation is noted in 15-20% of cases after 5 years. There is no clear consensus for Standard post-transplantation monitoring. A multi-center study has proposed a protocol using the RETREAT (Risk Estimation of Tumor Recurrence Post-Transplantation) scoring system for determining screening of HCC recurrence. This includes: AFP levels prior to transplant (max score of 3 for AFP >1000), vascular invasion (max score of 2 for any evidence of invasion), and sum of the diameters of HCC lesions (max score of 3 for sum >10). In our patient, with microvascular invasion, a score of 2 would standardize her to screening every 6 months for 2 years which was consistent with the monitoring she had.
The median time to HCC tumor recurrence is within 12-16 months post-transplantation, with over 75% occurring in first 2 years. Initial presentation of HCC recurrence as a direct gastrointestinal invasion is exceeding rare. There have been few case reports describing similar presentations as in our case, however, none have occurred after liver transplantation. Given its rarity, differential diagnosis of gastric ulcers in patients with history of HCC should include metastatic disease.
Figure: A. Gastric Ulcer B. Pancreatic Mass C. Lung Mass
Disclosures:
Alex Blachowicz indicated no relevant financial relationships.
Steven Hendler indicated no relevant financial relationships.
Marcel Ghanim indicated no relevant financial relationships.
Alex Blachowicz, MD, Steven Hendler, MD, Marcel Ghanim, MD. D0577 - A Rare Case of HCC Recurrence as a Bleeding Gastric Ulcer, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.