Lenox Hill Hospital - Northwell Health New York, NY
Victoria Garland, MD, Isabella Bergagnini, DO, Petros Benias, MD Lenox Hill Hospital - Northwell Health, New York, NY
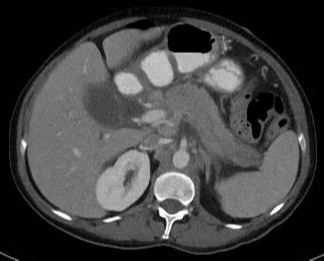
Introduction: Auto-immune pancreatitis (AIP) is an uncommon cause of recurrent pancreatitis characterized by chronic inflammation with lymphocytic infiltration on histology. It is further classified as type 1, IgG4 related and type 2, idiopathic duct-centric type, with a prevalence of 2% of chronic pancreatitis, affecting less than 1 per 100,000. We describe a case suspicious for AIP with pancreatic biopsy revealing metastatic lung adenocarcinoma.
Case Description/Methods: A 56-year-old female, former 10 pack year smoker with no medical history presented with complaints of worsening abdominal pain for one day. She notes a recent stay at an outside hospital for abdominal pain 5 days prior and was managed for gallstone pancreatitis. There, she underwent an ERCP with removal of biliary sludge and was planned for outpatient cholecystectomy. On this admission, a CT Abdomen/Pelvis revealed diffuse pancreatic enlargement with fullness most prominent at the head but no identifiable mass. Additionally, multiple enlarged retroperitoneal and mesenteric lymph nodes (LNs) were noted, measuring up to 2.5 cm. Radiographic findings were concerning for AIP versus malignancy. Labs were significant for a lipase 1078 and ANA 1:360 and subsequently managed for acute pancreatitis. IgG4 was at the upper limit of normal, 96 (2-96). On Day 5, she underwent an EGD/EUS, which revealed an enlarged pancreas, with no discrete mass as well as several mesenteric LNs, which were biopsied. Pathology revealed metastatic adenocarcinoma consistent with lung primary, PDL1 positive. An outpatient CT Chest revealed few pulmonary micronodules of unclear significance and borderline sized mediastinal LNs. She is currently following outpatient with thoracic oncology and undergoing further staging studies prior to initiation of treatment.
Discussion: Our patient presenting with clinical and radiographic features of AIP was diagnosed with metastatic lung cancer, a rare presentation of infiltrative metastasis mimicking autoimmune pancreatitis. While lung cancer is the 2nd leading cause of pancreatic metastasis, the literature has reported a few cases of lung cancer presenting as pancreatitis. Interestingly, 2 Japanese studies reported close temporality between AIP Type 1 diagnosis and cancer diagnosis, particularly with lung, stomach and prostate cancer, proposing the possibility that AIP can occur as an autoimmune paraneoplastic disease. Therefore, malignancy must be considered when evaluating for AIP and portends the necessity of endoscopic biopsy.
Figure: Enlarged heterogeneous pancreas, surrounding fat stranding and upper abdominal lymphadenopathy, suspicious for malignancy with co-existing pancreatitis.
Disclosures:
Victoria Garland indicated no relevant financial relationships.
Isabella Bergagnini indicated no relevant financial relationships.
Petros Benias indicated no relevant financial relationships.
Victoria Garland, MD, Isabella Bergagnini, DO, Petros Benias, MD. A0042 - An Unsuspecting Mimicker: Pancreatic Metastases Imitating as an Autoimmune Pancreatitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.