C0027 - Spontaneous Fistulization of Walled-Off Necrosis Into Duodenum Requiring Video-Assisted Retroperitoneal Debridement: A Rare Complication of Acute Necrotizing Pancreatitis
University of Puerto Rico School of Medicine Internal Medicine Program San Juan, Puerto Rico
Paola Laracuente Roman, MD1, Gabriela M. Negron-Ocasio, MD2, Juan G. Feliciano-Figueroa, MD3, Juan C. Santiago-Gonzalez, MD2, Marcel Mesa, MD3, Viviana Blanco Rivera, MD3 1University of Puerto Rico School of Medicine Internal Medicine Program, San Juan, Puerto Rico; 2University of Puerto Rico Medical Sciences Campus, San Juan, Puerto Rico; 3University of Puerto Rico School of Medicine, San Juan, Puerto Rico
Introduction: Gastrointestinal fistulas are an uncommon complication of acute or chronic pancreatitis, with colonic and duodenal fistula occurring in 60.5% and 26% of cases, respectively. We present a case of a spontaneous fistulization between the walled-off pancreatic necrosis (WOPN) and the duodenal bulb.
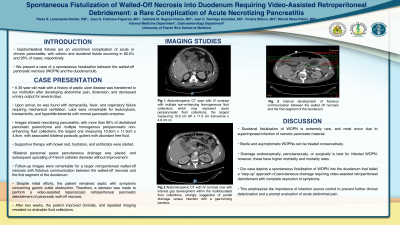
Case Description/Methods: A 35-year-old male with a history of peptic ulcer disease was transferred to our institution after developing abdominal pain, distension, and decreased urinary output for several days. Upon arrival, he was found with tachycardia, fever, and respiratory failure requiring mechanical ventilation. Laboratories were remarkable for leukocytosis, transaminitis, and hyperbilirubinemia with normal pancreatic enzymes. Images showed necrotizing pancreatitis, with more than 90% of devitalized pancreatic parenchyma and multiple homogenous peripancreatic non-enhancing fluid collections, the largest one measuring 10.9cm x 11.5cm x 4.8cm, with associated bilateral paracolic gutters with abundant free fluid. Supportive therapy with bowel rest, hydration, and antibiotics were started. Bilateral pararenal space percutaneous drainage was placed with subsequent upscaling of French catheter diameter without improvement. Follow-up images were remarkable for a larger retroperitoneal walled-off necrosis with fistulous communication between the walled-off necrosis and the first segment of the duodenum. Despite initial efforts, the patient remained septic with symptoms concerning gastric outlet obstruction. Therefore, a decision was made to perform a video-assisted laparoscopic retroperitoneal pancreatic debridement of pancreatic walled-off necrosis. After two weeks, the patient improved clinically, and repeated imaging revealed no drainable fluid collections.
Discussion: Duodenal fistulization of WOPN is extremely rare, and most occur due to superimposed infection of necrotic pancreatic material. Sterile and asymptomatic WOPNs can be treated conservatively. Drainage endoscopically, percutaneously, or surgically is best for infected WOPN; however, these have higher morbidity and mortality rates. Our case depicts a spontaneous fistulization of WOPN into the duodenum that failed a “step-up” approach of percutaneous drainage requiring video-assisted retroperitoneal debridement with complete resolution of symptoms. This emphasizes the importance of infection source control to prevent further clinical deterioration and a prompt evaluation of acute abdominal pain.
Disclosures:
Paola Laracuente Roman indicated no relevant financial relationships.
Gabriela Negron-Ocasio indicated no relevant financial relationships.
Juan Feliciano-Figueroa indicated no relevant financial relationships.
Juan Santiago-Gonzalez indicated no relevant financial relationships.
Marcel Mesa indicated no relevant financial relationships.
Viviana Blanco Rivera indicated no relevant financial relationships.
Paola Laracuente Roman, MD1, Gabriela M. Negron-Ocasio, MD2, Juan G. Feliciano-Figueroa, MD3, Juan C. Santiago-Gonzalez, MD2, Marcel Mesa, MD3, Viviana Blanco Rivera, MD3. C0027 - Spontaneous Fistulization of Walled-Off Necrosis Into Duodenum Requiring Video-Assisted Retroperitoneal Debridement: A Rare Complication of Acute Necrotizing Pancreatitis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.