Anya Ramrakhiani, 1, Ryan Gonzales, MD2 1Canterbury High School, Roanoke, IN; 2Fort Wayne Hematology and Oncology, Fort Wayne, IN
Introduction: Breast cancer can present as cervical lymph node enlargement causing dysphagia due to esophageal compression. We present a case of esophageal stenosis requiring placement of gastrostomy for administration of Palbociclib, which cannot be crushed or split.
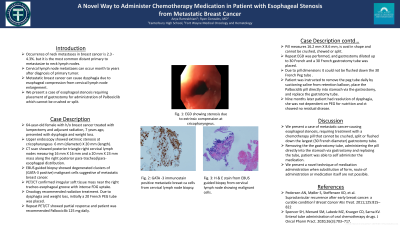
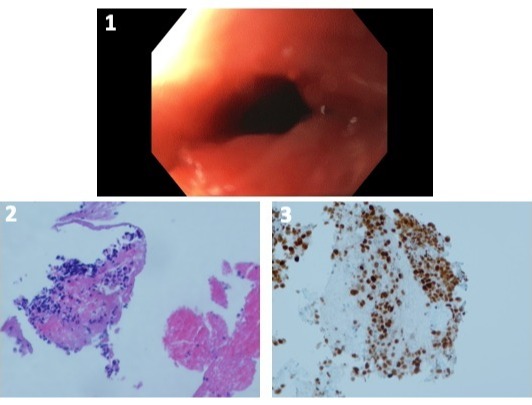
Case Description/Methods: 64 year-old female with history of breast cancer treated with lumpectomy and adjuvant radiation therapy, 7 years ago presented with dysphagia and weight loss. Upper endoscopy (fig. 1) showed extrinsic stenosis at cricopharyngeus 6 mm (diameter) X 2 cm (length). CT scan showed posterior triangle right cervical lymph nodes measuring 16 mm X 16 mm and a 20 mm X 23 mm mass along the right posterior para-tracheal/para-esophageal distribution. Endobronchial ultrasound guided biopsy was obtained. Pathology (fig. 2 and 3) showed degenerated clusters of (GATA-3 positive) malignant cells suggestive of metastatic breast cancer. PET/CT confirmed irregular soft tissue mass near the right tracheoesophageal groove with intense FDG uptake. There was regional metastatic lymphadenopathy in the right neck at the level IIA and IIIA regions. Oncology recommended radiation treatment. Due to dysphagia and weight loss, a 20 French PEG tube was placed using an ultraslim upper endoscope. Repeat PET/CT showed partial response and patient was recommended 125 mg Palbociclib tablet daily. The pill cannot be crushed or split and is oval, measuring 16.2 mm X 8.6 mm. Repeat upper endoscopy was performed, gastrostomy was dilated to 30 French, and a 30 French gastrostomy tube was placed. Due to the pill’s dimensions, it could not flush down the 30 French tube. Patient was instructed to remove the peg tube daily by suctioning saline from the retention balloon, place Palbociclib directly into the stomach via the gastrostomy, replace gastrostomy tube, and inflate the retention balloon with saline. Nine months later patient had resolution of dysphagia. She was not using her PEG tube and the CT scan showed no residual disease.
Discussion: We present a case of metastatic cancer causing esophageal stenosis, requiring treatment with a chemotherapy pill that cannot be crushed, split, or flushed down the largest (30 French diameter) available gastrostomy tube. Removing the gastrostomy tube, administering the pill directly into the stomach via gastrostomy, and replacing the tube, patient could self-administer the medication. We present a novel technique of medication administration when substitution of form, route of administration, and medication are not possible.
Figure: Fig. 1: EGD showing extrinsic stenosis at cricopharyngeus Fig. 2: Pathology with H&E stain showing presence of malignant cells Fig. 3: Pathology with GATA-3 immunostain positive metastatic breast cancer cells
Disclosures:
Anya Ramrakhiani indicated no relevant financial relationships.
Ryan Gonzales indicated no relevant financial relationships.
Anya Ramrakhiani, 1, Ryan Gonzales, MD2. B0731 - A Novel Way to Administer Chemotherapy Medication in a Patient With Esophageal Stenosis Secondary to Metastatic Breast Cancer, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.