San Ysidro Health/Scripps Mercy Chula Vista Hospital San Diego, CA
Andrew Bui, DO, Sharonya Shrivastava, MD San Ysidro Health/Scripps Mercy Chula Vista Hospital, San Diego, CA
Introduction: Chronic constipation in pediatric patients can lead to severe respiratory distress. We present an adult case of acute worsening of hypercarbic respiratory failure in the setting of obstipation.
Case Description/Methods: A 71 year-old man with a body mass index of 42, obesity hypoventilation syndrome on 2 liters of oxygen and ophthalmoplegia treated with intravenous immune globulin (IVIG) 1 year prior presented with acute generalized weakness. He had multiple falls and reported dropping items unintentionally for one day. Vital signs were notable for hypertension and oxygen saturation (SpO2) of 97% on 2 liters. His exam was remarkable for dysarthric speech, bilateral ptosis, inability to perform lateral gaze with improvement on ice pack test, and 1/5 strength globally. Laboratory values revealed a carbon dioxide (CO2) of 25 mmol/L, blood urea nitrogen was 35 mg/dL and creatinine of 1.6 mg/dL. An arterial blood gas showed a pH of 7.18, pCO2 of 58 mmHg and a negative inspiratory force of -40 cmHg. This finding was concerning for myasthenia gravis (MG) versus chronic inflammatory demyelinating polyneuropathy. He was transferred to the ICU for respiratory monitoring. He was started on pyridostigmine and IVIG with minimal improvement in his respiratory status. While monitoring his respiratory drive, his abdomen was noted to be distended. A chest X-ray demonstrated low lung volumes and an enlarged gastric bubble. Subsequent computed tomography of the abdomen and pelvis showed extensive colonic distention with fecal impaction. He was started on an aggressive bowel regimen including neostigmine with multiple bowel movements in response. His strength improved slightly and his respiratory status improved immediately. Acetylcholine receptor antibodies came back negative. He was discharged to a skilled nursing facility for rehabilitation.
Discussion: This case demonstrates how severe fecal impaction secondary to chronic constipation can contribute to respiratory distress in an adult, especially with possible concomitant neuromuscular disease. The increased abdominal distention from stool burden reduced functional capacity resulting in a restrictive pattern of respiratory failure. Interestingly, MG can cause Ogilvie's syndrome in rare cases as a result of autonomic dysmotility of the colon and can often be the initial presentation. It is hard to explain that despite his cardinal symptoms of MG, his neuropathy resolved not with immunosuppression, but with disimpaction.
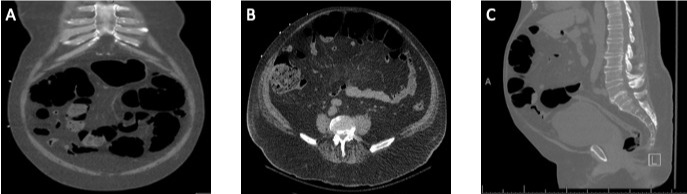
Figure: A. Computed tomography of the abdomen and pelvis without contrast (coronal view) showed extensive colonic distention with fecal impaction B. Computed tomography of the abdomen and pelvis without contrast (axial view) showing moderate colonic distention seen with transition point in the distal sigmoid colon with increased stool burden C. Computed tomography of the abdomen and pelvis without contrast (sagittal view) showing moderate colonic distention seen with transition point in the distal sigmoid colon with increased stool burden
Disclosures:
Andrew Bui indicated no relevant financial relationships.
Sharonya Shrivastava indicated no relevant financial relationships.
Andrew Bui, DO, Sharonya Shrivastava, MD. D0617 - Obstipation Masquerading as Myasthenia Gravis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.