UCLA, David Geffen School of Medicine Los Angeles, CA
Kush Fansiwala, MD1, Preeti Prakash, MD2, Christopher Coe, MD2, Guy A. Weiss, MD3 1UCLA, David Geffen School of Medicine, Los Angeles, CA; 2UCLA, Los Angeles, CA; 3University of California Los Angeles, Los Angeles, CA
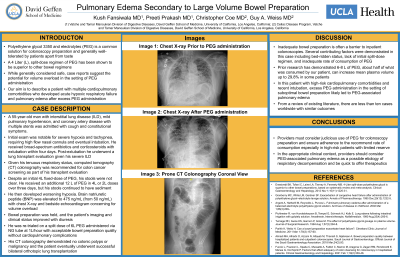
Introduction: Polyethylene glycol 3350 and electrolytes (PEG) is a perceived safe and commonly prescribed solution prior to colonoscopy, yet case reports suggest the potential for volume overload. We describe a patient with cardiopulmonary comorbidities who developed pulmonary edema and acute hypoxic respiratory failure (AHRF) due to PEG administration.
Case Description/Methods: A 55-year-old man with interstitial lung disease (ILD), mild pulmonary hypertension (pHTN), and coronary artery disease (CAD) with multiple coronary stents was admitted to our tertiary academic hospital with cough and constitutional symptoms. He had a brain natriuretic peptide (BNP) of 50 pg/mL, was found to be in AHRF and intubated due to labored breathing. He received broad-spectrum antibiotics and corticosteroids with clinical improvement and within four days was extubated. Given his severe ILD, he was evaluated for lung transplant. As part of this evaluation, mandatory colon cancer screening was needed in the form of computed tomography (CT) colonography. He had difficulty consuming Golytely at an appropriate rate. Despite 16 liters (L) of PEG over three days, the stools were not clear. He then re-developed hypoxia and tachypnea and BNP rise to 475 pg/mL. Chest X-ray (CXR) showed new bilateral opacities concerning for pulmonary edema. Echocardiography demonstrated an IVC greater than 2.0cm without respiratory variation consistent with volume overload. His bowel prep was held, and he was given diuretics with improvement in his respiratory status, BNP, and CXR. The patient was re-trialed on 6L PEG by nasogastric tube successfully without cardiopulmonary complications and his CT colonography showed no colonic polyps or malignancy. He eventually underwent successful bilateral orthotopic lung transplant.
Discussion: Prior research has shown that consumption of 6-8 L of PEG increases mean plasma volume by 5.88% on average, but up to 29.8% in some patients. In this case, our patient consumed double that amount of PEG, with subsequent increase in plasma volume, resulting in pulmonary edema and AHRF due to limited respiratory reserve from his severe ILD, pHTN, and CAD. Literature review shows less than ten cases worldwide with similar findings. In high-risk patients such as the one described, providers must consider judicious use of PEG for colonoscopy preparation and be quick to identify PEG-associated pulmonary edema as an etiology for respiratory decompensation.
Disclosures:
Kush Fansiwala indicated no relevant financial relationships.
Preeti Prakash indicated no relevant financial relationships.
Christopher Coe indicated no relevant financial relationships.
Guy Weiss: EverlyHealth – Advisory Committee/Board Member.
Kush Fansiwala, MD1, Preeti Prakash, MD2, Christopher Coe, MD2, Guy A. Weiss, MD3. A0124 - Pulmonary Edema Secondary to Large Volume Bowel Preparation, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.