University of California, Los Angeles Santa Monica, CA
Qiuxue T. Tan, MD1, Grant Chu, MD, MS2 1University of California, Los Angeles, Santa Monica, CA; 2University of California, Los Angeles, Torrance, CA
Introduction: Superior Mesentery Artery (SMA) Syndrome is a rare gastrovascular disorder due to narrowing of the space between the aorta and superior mesenteric artery, also known as aortomesenteric angle, which can compress the third part of the duodenum. Clinically, SMA syndrome in adults is associated with conditions, such a malignancy, trauma, extreme weight loss, or corrective spinal surgeries. We report a case of SMA syndrome in a patient without comorbidities to alert clinicians of the non-specific manifestations of this rare phenomenon.
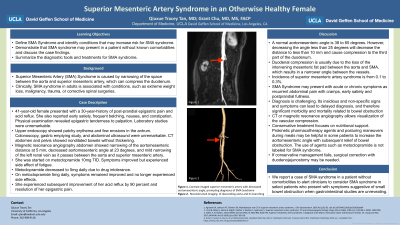
Case Description/Methods: A 41-year-old female presented with a 30-year-history of post-prandial epigastric pain and acid reflux. She also reported early satiety, frequent belching, nausea, and constipation. She denied vomiting, diarrhea, hematochezia, and weight loss. Physical examination revealed epigastric tenderness to palpation. Laboratory studies were unremarkable. Upper endoscopy showed patchy erythema and few erosions in the antrum consistent with gastritis. Colonoscopy, gastric emptying study, and abdominal ultrasound were unremarkable. CT abdomen and pelvis showed nondilated bowels without thickening. Magnetic resonance angiography abdomen showed narrowing of the aortomesenteric distance at 5 mm, decreased aortomesenteric angle at 23 degrees, and mild narrowing of the left renal vein as it passes between the aorta and superior mesenteric artery (Figure 1). SMA syndrome was diagnosed. She was started on metoclopramide 5mg twice a day with subsequent improvement of her acid reflux by 90 percent and resolution of her epigastric pain.
Discussion: SMA Syndrome may present with insidious non-specific signs and symptoms, which can lead to delayed diagnosis. When diagnosis is delayed, it can result in significant morbidity and mortality. Diagnosis is challenging. Gastric emptying studies may be falsely negative when the duodenum obstruction is relieved by positional changes. CT or magnetic resonance angiography allows visualization of the vascular compression. In mild cases without small bowel obstruction, prokinetic pharmacotherapy may help decrease symptoms. Surgical correction may be needed. Clinicians should consider SMA syndrome in select patients who present with symptoms suggestive of small bowel obstruction when gastrointestinal studies are unrevealing.
Figure: Decreased aortomesenteric angle of 23 degrees. A. Sagittal view. B. 3-dimensional reconstruction view.
Disclosures:
Qiuxue Tan indicated no relevant financial relationships.
Grant Chu indicated no relevant financial relationships.
Qiuxue T. Tan, MD1, Grant Chu, MD, MS2. D0645 - Superior Mesentery Artery Syndrome Presenting in an Otherwise Healthy Female, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.