Roel Sanchez Baez, MD, Andrew Bui, DO, Sharonya Shrivastava, MD San Ysidro Health, San Ysidro, CA
Introduction: We describe an immunocompromised individual with chronic diarrhea who developed an acute kidney injury in the setting of chronic Norovirus infection.
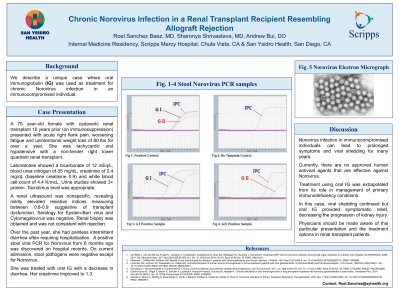
Case Description/Methods: A 75 year-old female with cadaveric renal transplant 10 years prior (on immunosuppression) presented with acute right flank pain, worsening fatigue and unintentional weight loss of 80 lbs for over a year. She was tachycardic and hypotensive with a non-tender right lower quadrant renal transplant. Laboratories showed a bicarbonate of 12 mEq/L, blood urea nitrogen of 35 mg/dL, creatinine of 2.4 mg/dL (baseline creatinine 0.9) and white blood cell count of 4.4 K/mcL. Urine studies showed 3+ protein and protein/creatinine ratio of 7,900 mg/g. Tacrolimus level was appropriate. A renal transplant ultrasound was nonspecific, revealing mildly elevated resistive indices measuring 0.8-0.9 suggestive of transplant dysfunction. Serology for Epstein-Barr virus and Cytomegalovirus was negative. Renal biopsy was obtained and was not consistent with either rejection or polyomavirus nephropathy. Patient reported episodes of watery diarrhea. Over the past year, she had painless intermittent diarrhea often requiring hospitalization. A positive stool viral PCR for Norovirus from 6 months ago was discovered on hospital records. Stool studies of C. difficile, Legionella, Shigella, Campylobacter, Salmonella, Cryptosporidium/Cyclospora and Giardia were negative and positive for Norovirus. She was treated with oral immunoglobulin (IG) with a decrease in diarrhea. Her creatinine improved to 1.3.
Discussion: Norovirus infection may progress to chronic infection after a solid organ transplant. Generally self-limiting, norovirus infection in immunocompromised individuals can lead to prolonged symptoms and viral shedding for many years. Minimal information is available in terms of prevalence of chronic Norovirus infection among solid organ transplant recipients. One study showed a prevalence of 4.6% among solid organ recipients. Of these, 22.8% developed chronic infection, with a median shedding period of 218 days. Currently, there are no approved human antiviral agents that are effective against Norovirus. Treatment using oral IG was extrapolated from its role in management of primary immunodeficiency conditions. In our patient, viral shedding continued but oral IG provided symptomatic relief, decreasing the progression of kidney injury. Physicians should be made aware of this particular presentation and treatment options in renal transplant patients.
Disclosures:
Roel Sanchez Baez indicated no relevant financial relationships.
Andrew Bui indicated no relevant financial relationships.
Sharonya Shrivastava indicated no relevant financial relationships.
Roel Sanchez Baez, MD, Andrew Bui, DO, Sharonya Shrivastava, MD. D0646 - Chronic Norovirus Infection in a Renal Transplant Recipient Resembling Allograft Rejection, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.