Vijay S. Are, MBBS1, Gaurav Suryawanshi, MD2, Guru Trikudanathan, MD2 1University of Minnesota, St. Paul, MN; 2University of Minnesota Medical Center, Minneapolis, MN
Introduction: In subjects with post Whipple anatomy, needing hepatobiliary drainage, ERCP is technically difficult and at times not feasible.
EUS guided gastrojejunostomy is an alternative method that is associated with less mortality, high success rate and less need for reintervention.
Case Description/Methods: 40-year-old Asian male with h/o T3N2 pancreatic adenocarcinoma and underwent who underwent Whipple procedure (5 months prior to presentation) who presented with fever, chills, epigastric pain, nausea and vomiting for the past two days.
Lab work was significant for elevated WBC and liver tests.
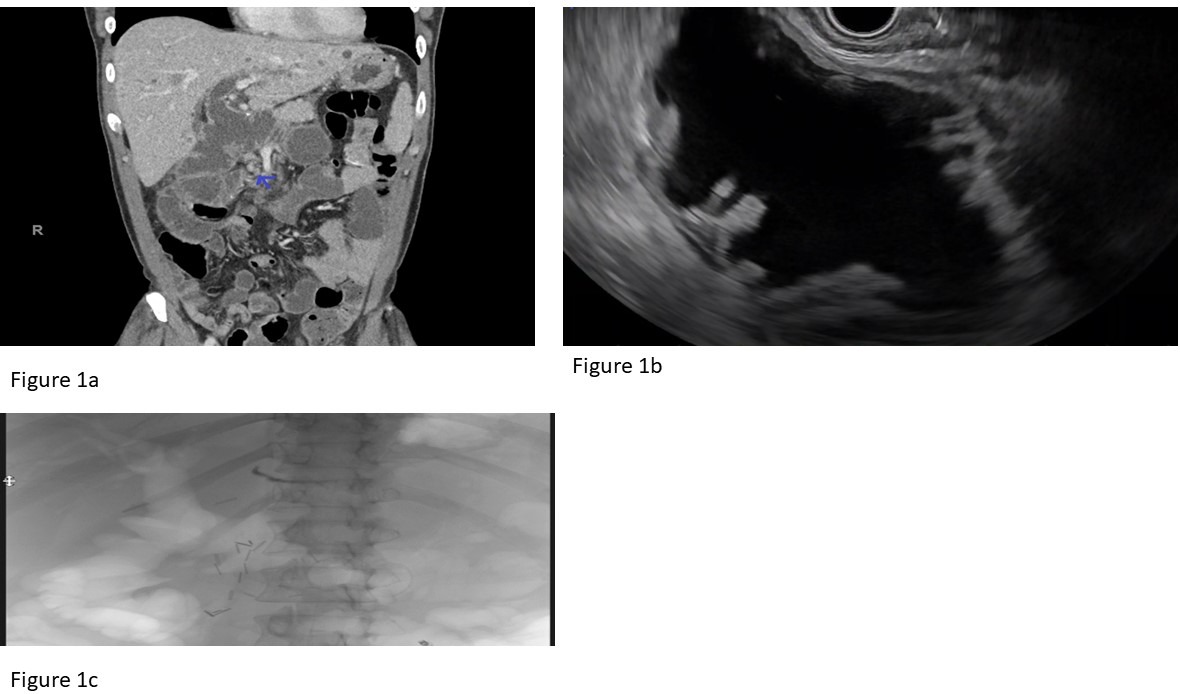
CT imaging revealed dilation of proximal jejunal (pancreaticobiliary limb) with transition point in region of surgical bed (Figure 1a). A diagnosis of obstructive jaundice due to pancreaticobiliary limb obstruction in the setting of post Whipple anatomy was made.
Two weeks ago, pt had endoscopic ultrasound guided assessment for concern for tumor recurrence and FNA biopsy was negative. During this procedure, there was mucosal trauma to the afferent limb that needed hemoclips to seal the defect.
Therefore, after a multidisciplinary consensus, further endoscopic manipulation of the afferent loop was felt to be harmful and so an EUS guided gastrojejunostomy was planned.
PROCEDURE:
After linear EUS scope was advanced into the stomach, a dilated loop of afferent jejunum was found adjacent to gastric antrum (Figure 1b). Once appropriate position in jejunum was identified, any interposed vessels were ruled out using Color Doppler imaging, a Lumen Apposing Metal Stent and cautery were introduced through working channel, and the stent was successfully deployed into afferent jejunal loop using a free hand technique. This resulted in drainage of copious amounts of dark bile into the stomach via LAMS. The distension of jejunal loop has resolved at the end of the procedure (Figure 1c).
Post procedurally, patient improved clinically. Leukocytosis and Liver tests have improved significantly. Pt continued to do well post discharge. CT scan obtained during follow up showed decompression of the afferent loop.
Discussion: Obstructive jaundice can occur due to afferent loop obstruction in a subjects with post Whipple anatomy. ERCP is technically difficult in this setting. EUS guided gastrojejunostomy is a promising option to relieve obstruction.
Figure: Figure 1a: Coronal CT imaging showing evidence of a post Whipple anatomy with a dilated pancreaticobiliary limb and upstream dilation of the hepaticojejunostomy anastomosis (Arrow points at the transition point) Figure 1b: Endoscopic ultrasound view showing a portion of the dilated proximal jejunum that is apposed to the stomach wall Figure 1c: Fluoroscopy image after stent deployment (air cholangiogram) indicating patency of the afferent loop and hepaticojejunostomy
Disclosures:
Vijay Are indicated no relevant financial relationships.
Gaurav Suryawanshi indicated no relevant financial relationships.
Guru Trikudanathan: Boston Scientific Corporation – Consultant.
Vijay S. Are, MBBS1, Gaurav Suryawanshi, MD2, Guru Trikudanathan, MD2. D0192 - EUS-Guided Gastrojejunostomy to Relieve Afferent Loop Obstruction, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.