University of Central Florida College of Medicine/HCA GME Consortium gainesville, FL
Raghav Bassi, MD1, Bilal Ashraf, MD2, Akiva Marcus, MD3 1University of Central Florida College of Medicine/HCA GME Consortium, Gainesville, FL; 2HCA/UCF Ocala Regional Medical Center, Ocala, FL; 3JFK Medical Center, Atlantis, FL
Introduction: Strongyloides stercoralis is a parasitic nematode mainly seen in immigrants and military personnel from endemic areas. Most cases in immunocompetent hosts are incidental findings or present with mild gastrointestinal (GI), respiratory or dermal symptoms. Co-infection with organisms like Campylobacter coupled with anatomical abnormalities such as a hiatal hernia can produce similar symptoms delaying diagnosis and treatment.
Case Description/Methods: A 75 year-old-woman presented with persistent watery diarrhea, nausea, dyspepsia, and non-bloody and non-bilious vomiting over the past five days. She also had an unintentional weight loss of 50 pounds over the past three months. She denied any recent travel, rashes, or fevers/chills. On presentation, she was hemodynamically stable with generalized abdominal tenderness on physical exam. CT of the abdomen revealed a moderately-sized hiatal hernia. Serologies were significant for normocytic anemia, thrombocytosis, and eosinophilia (white blood cell count 5300, eosinophils 6.6%). Stool studies were positive for Campylobacter and shewas started on azithromycin. She initially felt better and was subsequently discharged on azithromycin. She then presented three days later with complaints of nausea, and bloody emesis. Upper endoscopy with biopsy was done which showed a Los Angeles grade D reflux esophagitis and duodenitis. Histological evaluation revealed S. stercoralis in the duodenal mucosa (Figure 1). Initial ova and parasite cultures from a week ago further confirmed the diagnosis. She was then started on an extended course of ivermectin with a resolution of her symptoms and was discharged home.
Discussion: Campylobacter is an enteric gram-negative bacterium that also affects the GI tract and can mimic S. stercoralis infection clinically. Co-infection with this organism occurs due to its similar mode of transmission, however, there have only been a few cases documented in literature. Diagnosis is made by stool testing and serology, however, stool tests are only positive in 50-60% of cases. Eosinophilia may or may not be present. Clinicians should be aware that despite having underlying structural abnormalities such as a hiatal hernia, an EGD with biopsy is warranted to rule out infectious etiologies especially in the presence of eosinophilia as seen above. Early diagnosis and treatment are essential in preventing disseminated disease, especially in immunocompromised patients.
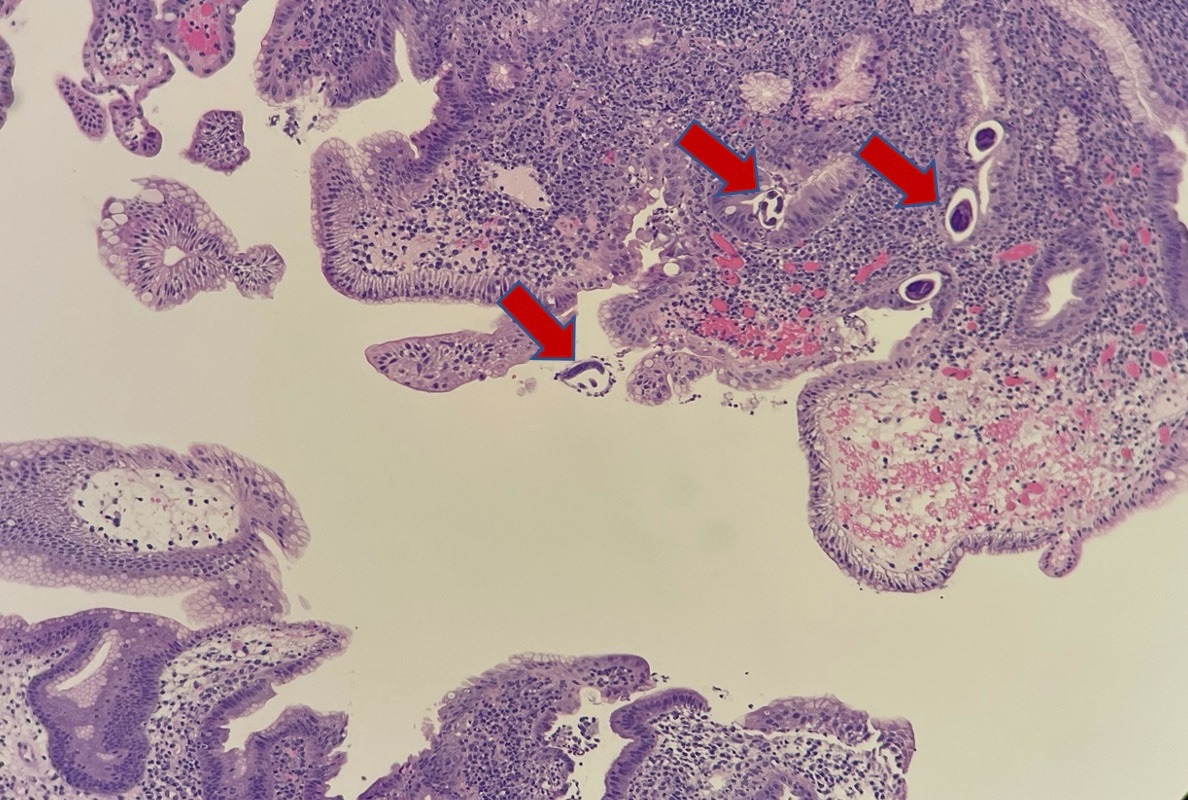
Figure: Figure 1: Hematoxylin and Eosin stain of the duodenum revealing acute duodenitis with associated Strongyloides stercoralis in the intestinal crypts and lumen.
Disclosures:
Raghav Bassi indicated no relevant financial relationships.
Bilal Ashraf indicated no relevant financial relationships.
Akiva Marcus indicated no relevant financial relationships.
Raghav Bassi, MD1, Bilal Ashraf, MD2, Akiva Marcus, MD3. D0667 - A Rare Case of Campylobacter and Strongyloides stercoralis Co-infection in an Immunocompetent Host, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.