Patrick J. Tempera, DO, Omar Tageldin, MD, Stephen Hasak, MD, MPH Albany Medical Center, Albany, NY
Introduction: Neuroendocrine tumor (NET) of the major duodenal papilla is a rare entity. However, NET of the minor duodenal papilla is even rarer and poorly studied. To our knowledge, only individual case reports and no comprehensive analyses are available in literature. We report a case of a somatostatin secreting NET located on the minor papilla with subsequent management outlined.
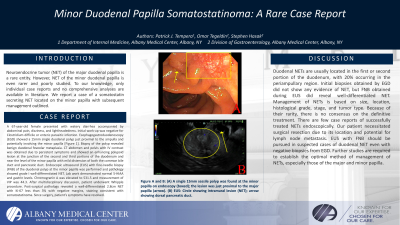
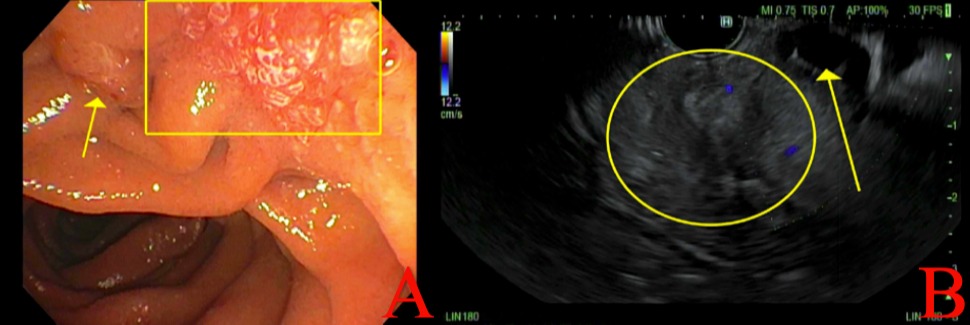
Case Description/Methods: A 67-year-old female presented with watery diarrhea accompanied by abdominal pain, dizziness, and lightheadedness. Initial work-up was negative for Clostridium difficile or enteric parasitic infection. Esophagogastroduodenoscopy (EGD) showed a 15mm single duodenal polyp just proximal to the ampulla and potentially involving the minor papilla [Figure 1]. Biopsy of the polyp revealed benign duodenal foveolar metaplasia. CT abdomen and pelvis with IV contrast was obtained due to persistent symptoms and showed an enhancing polypoid lesion at the junction of the second and third portions of the duodenum and near the level of the minor papilla with mild distension of both the common bile duct and pancreatic duct. Endoscopic ultrasound (EUS) with fine-needle biopsy (FNB) of the duodenal polyp at the minor papilla was performed and pathology showed grade I well-differentiated NET. Lab work demonstrated normal 5-HIAA and gastrin levels. Chromogranin A was elevated to 531.5 and measurement of VIP was 44.3. After multidisciplinary discussion, patient underwent Whipple procedure. Post-surgical pathology revealed a well-differentiated 2.8cm NET with Ki-67 less than 3% with negative margins, staining consistent with somatostatinoma. Since surgery, patient’s symptoms have resolved.
Discussion: Duodenal NETs are usually located in the first or second portion of the duodenum, with 20% occurring in the periampullary region. Initial biopsies obtained by EGD did not show any evidence of NET, but FNB obtained during EUS did reveal well-differentiated NET. Management of NETs is based on size, location, histological grade, stage, and tumor type. Because of their rarity, there is no consensus on the definitive treatment. There are few case reports of successfully treated NETs endoscopically. Our patient necessitated surgical resection due to its location and potential for lymph node metastasis. EUS with FNB should be pursued in suspected cases of duodenal NET even with negative biopsies from EGD. Further studies are required to establish the optimal method of management of NETs, especially those of the major and minor papilla.
Figure: Figure-1: (A) A single 15mm sessile polyp was found at the minor papilla on endoscopy (boxed); the lesion was just proximal to the major papilla (arrow). (B) EUS: Circle showing intramural lesion (NET); arrow showing dorsal pancreatic duct.
Disclosures:
Patrick Tempera indicated no relevant financial relationships.
Omar Tageldin indicated no relevant financial relationships.
Stephen Hasak indicated no relevant financial relationships.
Patrick J. Tempera, DO, Omar Tageldin, MD, Stephen Hasak, MD, MPH. D0669 - Minor Duodenal Papilla Somatostatinoma: A Rare Case Report, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.