Aleena Moin, DO1, Harrison R. Malcolm, JD, DO2, Bradley D. Confer, DO1 1Geisinger Medical Center, Danville, PA; 2Geisinger Health System, Danville, PA
Introduction: Signet cell carcinoma is a distinct subtype of gastric cancer diagnosed via the characteristic presence of cytoplasmic mucin and an eccentrically displaced nucleus. In recent years, the incidence of this cancer has been increasing.
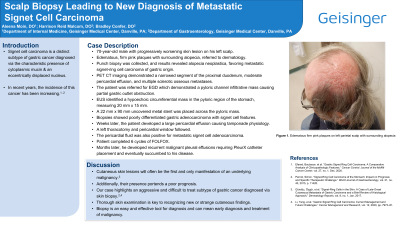
Case Description/Methods: A 70-year-old male consulted his PCP for a progressively worsening skin lesion on his left scalp. The physical exam shows edematous, firm pink plaques with surrounding alopecia for which he was referred to dermatology. The leading differential was scarring alopecia or sarcoidosis. Subsequent punch biopsy was collected, and results revealed alopecia neoplastica, favoring metastatic signet-ring cell carcinoma of gastric origin. Oncological workup was pursued. Whole-body PET CT imaging demonstrated a narrowed segment of the proximal duodenum, moderate pericardial effusion, and multiple sclerotic osseous metastases.
The patient was referred for an EGD which demonstrated a pyloric channel infiltrative mass causing partial gastric outlet obstruction. An upper EUS identified a hypoechoic circumferential mass in the pyloric region of the stomach, measuring 20 mm x 15 mm. Given the developing gastric outlet obstruction, a 22 mm x 90 mm uncovered metal stent was placed across the pyloric mass. Biopsies showed poorly differentiated gastric adenocarcinoma with signet cell features.
A couple of weeks later, the patient developed atrial fibrillation with evidence of a large pericardial effusion causing tamponade physiology. A left thoracotomy and pericardial window followed. The pathology specimen of pericardial fluid was also positive for metastatic signet cell adenocarcinoma. The patient completed 6 cycles of FOLFOX under the guidance of oncology. A few months later, he developed recurrent malignant pleural effusions requiring PleurX catheter placement. However, his dyspnea remained progressive, and the patient eventually succumbed to his disease.
Discussion: Cutaneous skin lesions are often the first and only manifestation of an underlying malignancy. Additionally, their presence portends a poor prognosis. Our case highlights an aggressive and difficult-to-treat subtype of gastric cancer diagnosed after a scalp biopsy. A thorough skin examination is key to recognizing new or strange cutaneous findings. Skin biopsy is an easy and effective tool for diagnosis and leads to early recognition and treatment of potential malignancies.
Figure: Figure 1. This image showcases edematous, firm pink-colored plaques with surrounding alopecia located over the patient's left temporoparietal scalp region.
Disclosures:
Aleena Moin indicated no relevant financial relationships.
Harrison Malcolm indicated no relevant financial relationships.
Bradley Confer indicated no relevant financial relationships.
Aleena Moin, DO1, Harrison R. Malcolm, JD, DO2, Bradley D. Confer, DO1. D0697 - Scalp Biopsy Leading to New Diagnosis of Metastatic Signet Cell Carcinoma, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.