University of Texas Health Science Center San Antonio, TX
Award: Presidential Poster Award
David J. Restrepo, MD1, Farah H. Ladak, MD1, Carl L. Kay, MD2, Patrick Snyder, MD3, Juan Echavarria, MD1 1University of Texas Health Science Center, San Antonio, TX; 2Brooke Army Medical Center, JBSA Fort Sam Houston, TX; 3UT Health San Antonio, San Antonio, TX
Introduction: Sigmoid volvulus is a rare cause of bowel obstruction in the general population and particularly in pregnancy. Here, we present a case of a young woman in her third trimester presenting with acute sigmoid volvulus.
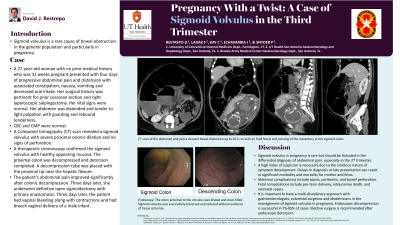
Case Description/Methods: A 27-year-old woman with no prior medical history who was 31 weeks pregnant presented with four days of progressive abdominal pain and distension with associated obstipation, nausea, vomiting and decreased oral intake. Her surgical history was pertinent for prior cesarean section and right laparoscopic salpingectomy. Her vital signs are normal. Her abdomen is distended and tender to light palpation with guarding and rebound tenderness. CBC and CMP are within normal limits. A computed tomography (CT) scan of the abdomen and pelvis showed large bowel distension up to 10.5 cm with air fluid levels and twisting of the mesentery at the sigmoid colon. Based on these findings, she was diagnosed with sigmoid volvulus.
The patient was emergently taken to the operating room for endoscopic sigmoid volvulus reduction. A therapeutic colonoscopy revealed a sigmoid volvulus with health appearing mucosa which was successfully traversed and detorsion was performed. A nasogastric tube was placed in the rectum with the proximal tip near the hepatic flexure for decompression.
The patient’s abdominal pain improved significantly after colonic decompression. Three days later, she underwent definitive open sigmoidectomy with primary anastomosis. Three days later, the patient had vaginal bleeding along with contractions and had breech vaginal delivery of a male infant.
Discussion: Sigmoid volvulus in pregnancy is rare but should be included within the differential diagnosis for abdominal pain as a delay in diagnosis or late presentation can result in significant morbidity and mortality for mother and fetus. Delays in diagnosis are associated with high rates of morbidity and mortality for the mother and fetus. Maternal complications include sepsis, peritonitis, and bowel perforation. Fetal complications include pre-term delivery, intrauterine death, and neonatal sepsis. Endoscopic decompression is successful in 75-95% of cases. Elective surgery is recommended after endoscopic detorsion. Finally, it is important to have a multi-disciplinary approach with colorectal surgeons and obstetricians in the management of sigmoid volvulus in pregnancy.
Figure: Sagittal view of abdomen and pelvis CT Scan
Disclosures:
David Restrepo indicated no relevant financial relationships.
Farah Ladak indicated no relevant financial relationships.
Carl Kay indicated no relevant financial relationships.
Patrick Snyder indicated no relevant financial relationships.
Juan Echavarria indicated no relevant financial relationships.
David J. Restrepo, MD1, Farah H. Ladak, MD1, Carl L. Kay, MD2, Patrick Snyder, MD3, Juan Echavarria, MD1. D0143 - Pregnancy With a Twist: A Case of Sigmoid Volvulus in the Third Trimester, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.