Patrick Lazarczyk, DO1, Suhind Kodali, MD1, Eric M. Sieloff, MD1, Marc S. Piper, MD, MSc2 1Ascension Providence Hospital, Southfield, MI; 2Ascension Providence, Southfield, MI
Introduction: Granular cell tumors (GCTs) are thought to originate from Schwann cells and rarely affect the gastrointestinal (GI) tract. Reported cases of GI involvement indicate the esophagus is most affected, while the colon is rarely involved. The majority of GCTs are benign, though approximately 1% can be malignant. We present a rare case of esophageal GCT with metastases to the lung and cecum.
Case Description/Methods: A 59-year-old female with history of colon polyps presented to our gastroenterology office for surveillance colonoscopy. She was incidentally found to have iron-deficiency anemia, and double endoscopy was arranged. Esophagogastroduodenoscopy found a 3cm submucosal esophageal mass in the upper esophagus with multiple non-bleeding gastric angiodysplastic lesions, and one duodenal lesion, which were treated with argon plasma coagulation. A colonoscopy was aborted due to poor preparation.
The esophageal mass biopsy found a granular cell tumor with S100 positivity. She was referred for endoscopic submucosal dissection (ESD) for her esophageal mass but was unfortunately lost to follow up. The patient underwent a series of imaging, including a PET-CT scan showing a 7mm nodule in the left upper lung lobe with minimal metabolic activity. Three months later, a CT thorax without contrast showed enlargement of the left upper lobe nodule to 1cm with multiple other small nodules noted. The patient underwent an endobronchial ultrasound with lung biopsy yielding granular cell tumor.
Repeat colonoscopy ultimately found a 20mm polyp in the cecum with pathology again identifying a granular cell tumor. Repeat PET-CT scan re-demonstrated the mildly FDG avid left upper lobe nodule measuring 1.1cm but also found a focal area of increased activity in the left anorectal wall. The patient began to experience significant dysphagia and was again referred for ESD which will be completed in the near future.
Discussion: Granular cell tumors may present localized or with metastases to various organs. The diagnosis of GCT is made via histopathology. In our case, an esophageal GCT was found with suspected spread to the lungs and cecum.
Although most tumors are benign with a favorable prognosis, patients may develop symptoms such as dysphagia, cough, abdominal pain, nausea, or chest pain, especially when involving the GI tract. The definitive treatment is surgical or endoscopic removal, as chemotherapy and radiation are rarely effective. Long-term surveillance is essential as tumors may recur following resection.
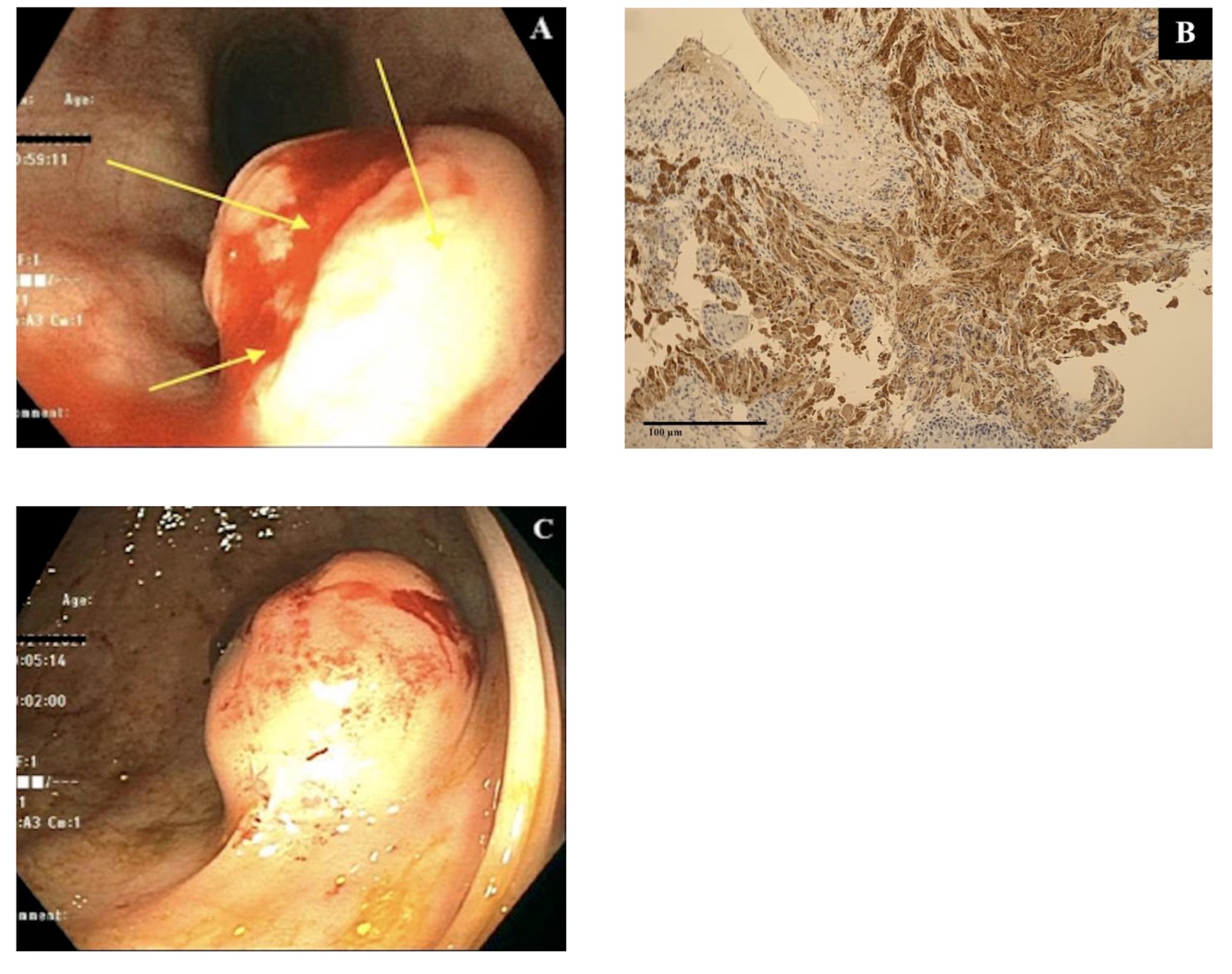
Figure: Figure 1: Upper endoscopy imaging showing 3cm submucosal mass in upper esophagus (A). Immunohistochemistry image showing positive S100 staining of esophageal mass (B). Colonoscopy imaging showing 20mm polypoid lesion in the cecum (C).
Disclosures:
Patrick Lazarczyk indicated no relevant financial relationships.
Suhind Kodali indicated no relevant financial relationships.
Eric Sieloff indicated no relevant financial relationships.
Marc Piper indicated no relevant financial relationships.
Patrick Lazarczyk, DO1, Suhind Kodali, MD1, Eric M. Sieloff, MD1, Marc S. Piper, MD, MSc2. B0298 - A Rare Case of Metastatic Esophageal Granular Cell Tumor, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.