Manavi Bhagwat, MD1, Michelle Godbee, MD1, Ali Keshavarzian, MD2 1Rush University Medical Center, Chicago, IL; 2Rush Center for Integrated Microbiome and Chronobiology Research, Chicago, IL
Introduction: Increased cancer risk in inflammatory bowel disease (IBD) is thought to be due to immunosuppression from biologic therapy and/or inflammation. Women with IBD have an increased risk of melanoma and adenocarcinoma of the small bowel and colon, and those that are on an immunosuppressive regimen that includes azathioprine have an additional increased risk of lymphoma and squamous cell carcinoma of the skin and cervix. Here we present a case of a patient with an atypical and rare malignancy, whose diagnosis was delayed due to overlap in the symptoms of the malignancy and her known IBD diagnosis.
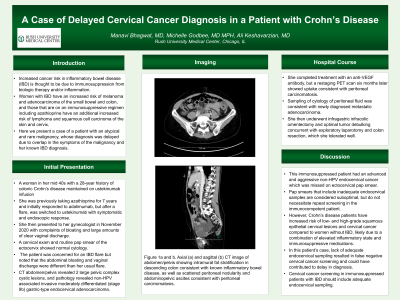
Case Description/Methods: A woman in her mid 40s with a 28-year history of colonic Crohn’s disease maintained on ustekinumab injection. She was previously taking azathioprine for 7 years and initially responded to adalimumab, but after a flare, was switched to ustekinumab with symptomatic and endoscopic response. She then presented to her gynecologist in November 2020 with complaints of bloating and large amounts of clear vaginal discharge. A cervical exam and routine pap smear of the ectocervix showed normal cytology. Eight months later, the patient presented to her gastroenterologist with worsening bloating, hematochezia, left lower quadrant pain, and persistent vaginal discharge. The patient was concerned for an IBD flare, but noted that the abdominal bloating and vaginal discharge were different than her usual flare. After CT abdomen/pelvis revealed 2 large pelvic complex cystic lesions, her biologic was stopped and she underwent a hysterectomy with bilateral salpingo-oophorectomy. Pathology revealed non-HPV associated invasive moderately differentiated gastric-type endocervical adenocarcinoma. She completed treatment with an anti-VEGF antibody, but a restaging PET scan six months later showed uptake consistent with peritoneal carcinomatosis.
Discussion: This immunosuppressed patient had an advanced and aggressive non-HPV endocervical cancer which was missed on ectocervical pap smear. Pap smears that include inadequate endocervical samples are considered suboptimal, but are usually not grounds for further testing in the average patient. However, Crohn’s disease patients have increased risk of low- and high-grade squamous epithelial cervical lesions and cervical cancer compared to women without IBD, likely due to a combination of elevated inflammatory state and immunosuppressive medications. Cervical cancer screening in immunosuppressed patients with IBD should include adequate endocervical sampling.
Disclosures:
Manavi Bhagwat indicated no relevant financial relationships.
Michelle Godbee indicated no relevant financial relationships.
Ali Keshavarzian indicated no relevant financial relationships.
Manavi Bhagwat, MD1, Michelle Godbee, MD1, Ali Keshavarzian, MD2. B0430 - A Case of Delayed Cervical Cancer Diagnosis in a Patient With Crohn’s Disease, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.