Suaka Kagbo-Kue, MBBS1, Blanca Lizaola-Mayo, MD1, Jaime Bering, MD2, David Chascsa, MD1 1Mayo Clinic, Phoenix, AZ; 2Mayo Clinic, Scottsdale, AZ
Introduction: Esophageal varices (EV) are a complication of portal hypertension. Over time, EV enlarge and may spontaneously rupture, leading to bleeding and possibly death with a high mortality rate of up to 20%. Esophageal variceal ligation (EVL) is used for prophylaxis, as well as treatment of acute variceal bleeding with the goal of eradicating varices. EVL is an effective therapy with rare but serious complications including bleeding, ulcers, strictures, and rarely acute obstruction. Amongst the few reported cases of esophageal obstruction, treatment has varied but mostly involved conservative management or band removal. We present a case of post EVL acute esophageal obstruction that was uniquely treated with band removal and esophageal stenting.
Case Description/Methods: A 79yo female with nonalcoholic steatohepatitis cirrhosis and a MELD-Na of 12, complicated by portal hypertension and EV status post previous banding one year prior came to the emergency room two days after esophagogastroduodenoscopy (EGD) for routine EV surveillance with placement of two bands resulting in complete eradication. She presented with one episode of hematemesis and dysphagia to liquids, and regurgitation; denied odynophagia and chest pain. Hematologic parameters were at baseline.
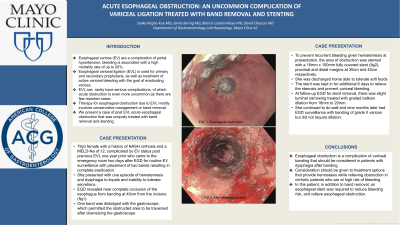
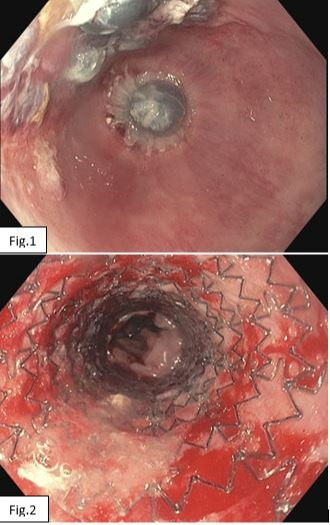
EGD revealed near-complete occlusion of the esophagus from banding at 40cm from the incisors (fig1). One band was dislodged with the gastroscope, which permitted the obstructed area to be traversed after downsizing the gastroscope. No active bleeding was evident. To prevent recurrent bleeding given hematemesis at presentation, the area of obstruction was stented with a 16mm x 100mm fully covered stent (fig2), proximal and distal margins at 30cm and 40cm respectively.
She was discharged home after 24 hours able to tolerate soft foods. The stent was kept for seven days. At follow-up EGD for stent removal, there was slight luminal narrowing treated with graded balloon dilation from 18mm to 20mm. She continued to do well and nine months later had EGD surveillance with banding of grade II varices only.
Discussion: Acute esophageal obstruction, though rare, is a complication of variceal banding that should be considered in patients with dysphagia after banding. This is a case that required innovative thinking and priority to treatment options that provide hemostasis while relieving obstruction in a cirrhotic patient with a high risk of bleeding.
Figure: Fig 1. Near complete occlusion of esophagus Fig 2. After placement of esophageal stent
Disclosures:
Suaka Kagbo-Kue indicated no relevant financial relationships.
Blanca Lizaola-Mayo indicated no relevant financial relationships.
Jaime Bering indicated no relevant financial relationships.
David Chascsa indicated no relevant financial relationships.
Suaka Kagbo-Kue, MBBS1, Blanca Lizaola-Mayo, MD1, Jaime Bering, MD2, David Chascsa, MD1. B0594 - Acute Esophageal Obstruction: An Uncommon Complication of Variceal Ligation Treated With Band Removal and Stenting, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.