Alameda Health System - Highland Hospital Oakland, CA
Sindhu Chadalawada, MD1, Christina Chou, MD2 1Alameda Health System - Highland Hospital, Oakland, CA; 2Alameda Health System – Highland Hospital, Oakland, CA
Introduction: Colorectal cancer (CRC) is the third leading cause of cancer related mortality worldwide. The U.S. Preventative Services Task Force guidelines recommend screening for average risk patients at age 45, and modalities include stool-based or direct visualization tests. We report a presentation of Stage IV colorectal adenocarcinoma in the setting of three annual negative fecal immunochemical testing (FIT) tests.
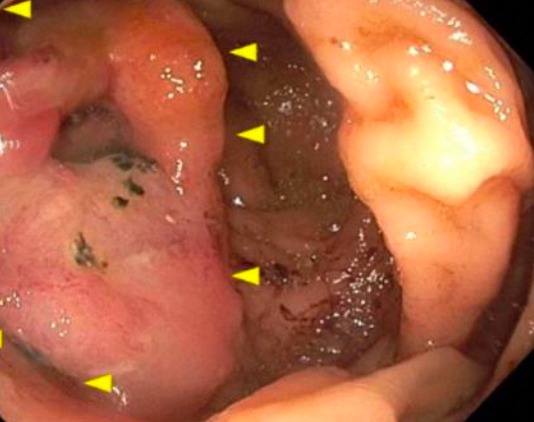
Case Description/Methods: A 67-year-old woman presented with shortness of breath, unintentional weight loss, and abdominal pain. She denied hematochezia or melena. Physical exam was notable for pallor and right upper quadrant pain. Initial laboratory data showed normocytic anemia with a hemoglobin 10.1 g/dL, alkaline phosphatase 610 U/L, aspartate aminotransaminase 116 U/L, alanine aminotransaminase 67 U/L. Computed tomography of the chest, abdomen, and pelvis revealed a normal colon and extensive metastatic disease in the liver and lungs with bilateral subsegmental pulmonary emboli. Chart review was notable for negative FIT tests in 2017, 2018, and 2020, performed within a year of this presentation. Further workup was significant for elevated carcinogenic embryonic antigen 1470 ng/mL, and normal alpha-fetoprotein and cancer antigen 19-9 levels. Colonoscopy revealed an infiltrating, ulcerated, semi-circumferential mass at the ileo-cecal valve and ascending colon (Figure 1). Pathology demonstrated moderately differentiated invasive colonic adenocarcinoma with malignant glands infiltrating a desmoplastic stroma. Immunohistochemistry did not show any microsatellite instability changes.
Discussion: One study showed FIT testing was 73.8% sensitive for detecting Stage I-III CRC, however, sensitivities dropped with advanced precancerous lesions and sessile serrated polyps to 23.8% and 5.1% respectively. Another retrospective cohort looking at six consecutive rounds of FIT testing demonstrated lower accuracy of detecting proximal colon cancers compared to distal cancers (0.45 vs 0.73; P< 0.001). Lower cut off values of qualitative FIT correlated with better sensitivities, however, specificity declined. Although FIT testing is able to detect the majority of colorectal cancers, it has decreased accuracy and sensitivity in advanced precancerous lesions, sessile serrated polyps, and proximal (right) colon lesions. Colonoscopy is considered gold standard and further guidelines should recommend a standardized cut off value to help improve screening efficacy.
Figure: Figure 1. Large fungating mass in the ascending colon and ileo-cecal valve
Disclosures:
Sindhu Chadalawada indicated no relevant financial relationships.
Christina Chou indicated no relevant financial relationships.
Sindhu Chadalawada, MD1, Christina Chou, MD2. B0182 - FIT or Unfit: Advanced Colon Cancer Screening, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.