Qitan Huang, DO1, Sean-Patrick Prince, MD, MPH2, Denisse Camille Dayto, MD1, Arjun Grewal, MD3, Siddarth Mathur, MD1 1HCA Florida Citrus Hospital, Inverness, FL; 2University of Miami/Holy Cross Health, Inverness, FL; 3Lincoln Memorial University DeBusk College of Osteopathic Medicine, Harrogate, TN
Introduction: Primary colorectal lymphomas are rare and account for 0.3% of all large intestinal malignancies, with Diffuse Large B-Cell Lymphoma (DLBCL) representing the most common subtype. We present a case of primary colonic DLBCL that was diagnosed after surgical resection of the sigmoid colon.
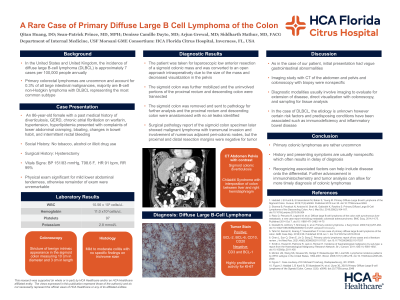
Case Description/Methods: An 86-year-old Caucasian female with a past medical history of diverticulosis and atrial fibrillation presented to the emergency department complaining of abdominal cramping and rectal bleeding. Physical examination was significant for mild abdominal tenderness and vital signs revealed blood pressure of 151/83 mmHg. Laboratory investigations were significant for white blood cell count of 10.56 x 10^3 cells/uL and potassium 2.8 mmol/L. Abdominal and pelvic computed tomography with contrast revealed sigmoid colonic diverticulosis with interposition of colon between liver and right hemidiaphragm. The patient underwent colonoscopy that showed a stricture of benign intrinsic appearance in the sigmoid colon measuring 10 cm in diameter and 3 cm in length. Histological analysis of tissue biopsies taken at that time were only significant for mild to moderate colitis. After colonoscopy, she was taken for laparoscopic low anterior resection of the sigmoid colonic mass that was later converted to an open approach due to the size of the mass. After the incision was extended, the sigmoid colon was further mobilized and the uninvolved portions of the proximal rectum and descending colon were transected. After the sigmoid colon was removed and sent to pathology, the proximal rectum and descending colon were anastomosed with no air leaks identified. Pathology report of the surgical specimen later showed malignant lymphoma with transmural invasion and involvement of numerous adjacent pericolonic nodes with negative tumor margins. Immunostains revealed the tumor to be positive for BCL-2, BCL-6, CD10, and CD20 but negative for CD3 and BCL-1. High proliferative activity was discerned for KI-67 staining in 90% of tumor cells; all evidence supporting the diagnosis of DLBCL. After an uneventful postoperative period and clinical improvement, the patient was discharged to home for close follow-up.
Discussion: Primary colonic lymphomas are rare and usually present with nonspecific symptoms. Although in the case discussed, the patient did not present with any obvious predisposing conditions for DLBCL, further data is necessary to determine other possible associations and develop a standardized treatment regimen.
Disclosures:
Qitan Huang indicated no relevant financial relationships.
Sean-Patrick Prince indicated no relevant financial relationships.
Denisse Camille Dayto indicated no relevant financial relationships.
Arjun Grewal indicated no relevant financial relationships.
Siddarth Mathur indicated no relevant financial relationships.
Qitan Huang, DO1, Sean-Patrick Prince, MD, MPH2, Denisse Camille Dayto, MD1, Arjun Grewal, MD3, Siddarth Mathur, MD1. E0107 - A Rare Case of Primary Diffuse Large B Cell Lymphoma of the Colon, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.