University of Arizona College of Medicine Phoenix, AZ
Majd Aboona, BS1, Erica Turse Dailey, DO, MPH2, William Anderson, MD2, Shifat Ahmed, MD2 1University of Arizona College of Medicine, Phoenix, AZ; 2Creighton University School of Medicine (Phoenix) Program/Saint Joseph's Hospital Medical Center, Phoenix, AZ
Introduction: Pneumatosis cystoides intestinalis (PCI) is characterized by the presence of gaseous cysts containing nitrogen, hydrogen, and carbon dioxide. This rare condition can be idiopathic (15% of cases), or secondary to another medical condition (85% of cases). The most common symptoms attributed to PCI have been diarrhea, bloody stools, abdominal pain, constipation, weight loss and tenesmus. The most common histologic findings associated with PCI includes gas cysts, multinucleated giant cells, macrophages, and pericystic inflammatory changes. Primary PCI typically creates a cystic pattern within the intraluminal wall and secondary causes creates a linear pattern. It is important to recognize this disease entity given the endoscopic appearance similar to other lesions such as sessile serrated adenomas.
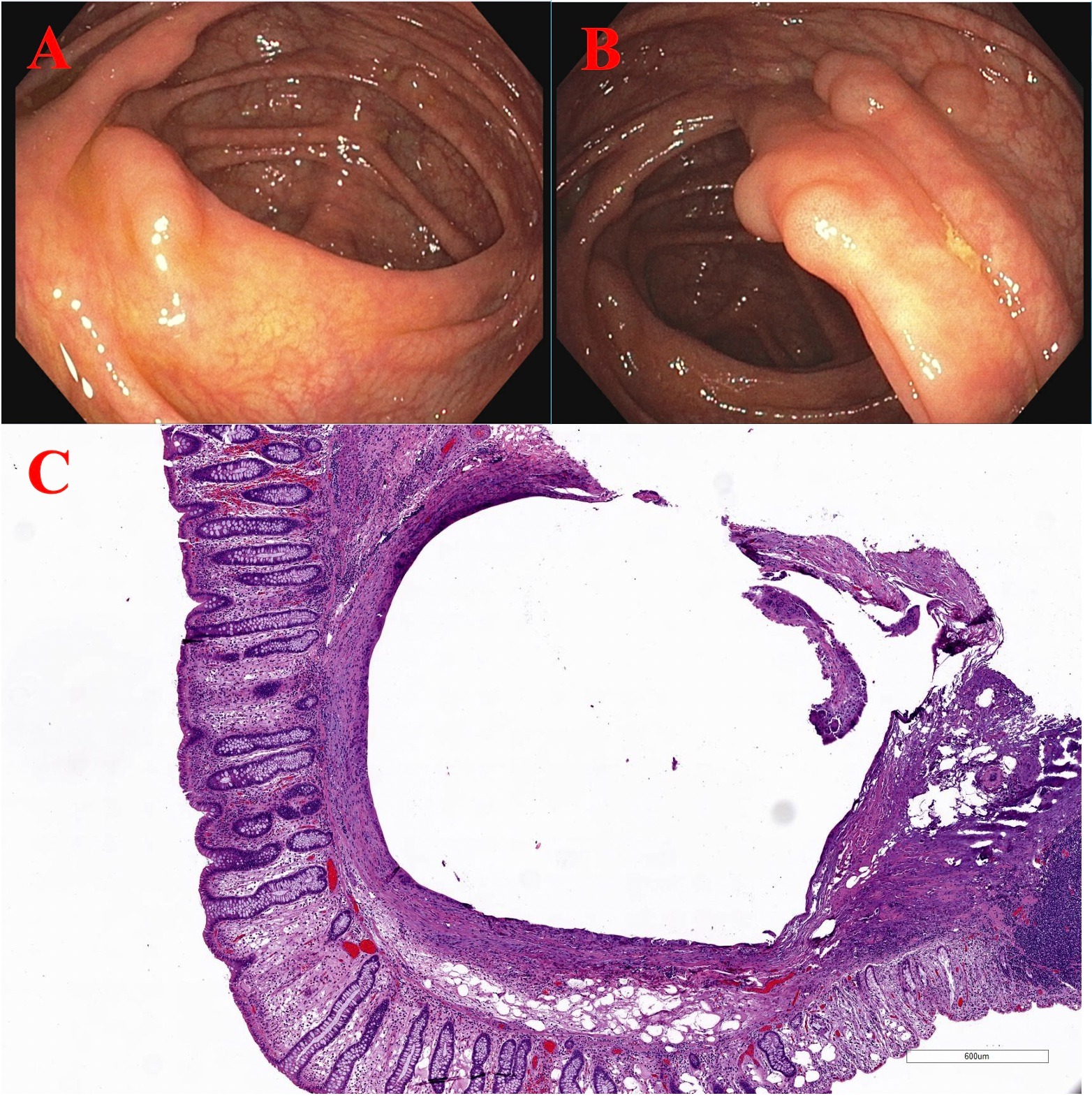
Case Description/Methods: A forty-two year old African male underwent colonoscopy for new constipation and a first degree relative history of colorectal cancer at age 45. The colonoscopy performed revealed a 12mm sessile polypoid lesion on the ileocecal valve (Image A), with a normal terminal ileum, which underwent endoscopic resection using snare polypectomy. Five additional polypoid lesions seen in the ascending colon ranging from 5-12mm in size (Image B) were removed with snare polypectomy. Pathology of these lesions showed empty appearing submucosal cystic structures with peripheral foreign body, and giant cell reaction (Image C) diagnostic for localized PCI.
Discussion: PCI is not well understood and can be multifactorial from a mechanical defect, gas produced from bacteria, or gas from a pulmonary source. Some patients may have symptoms of abdominal pain, obstruction or bleeding but most individuals are asymptomatic and rely on endoscopy or imaging for diagnosis. Although many cases are asymptomatic, complications include obstructions from gaseous cysts, and rarely, rupture of these cysts can cause pneumoperitoneum. This patient’s constipation could be related to his underlying diagnosis of PCI. In the management of these patients, oxygen therapy is considered the first approach. It is thought that cysts release gases within them and refill with oxygen that is then metabolized resulting in cyst resolution. Second line therapy is surgical treatment and is required in the setting of pneumoperitoneum. In patients with nonspecific abdominal symptoms, an endoscopy could be warranted to assess for primary PCI which if left untreated can cause complications.
Figure: Image A: 12mm sessile polypoid lesion on the ileocecal valve Image B: Five polypoid lesions ranging from 5-12mm in the ascending colon Image C: Microscopic image showing empty appearing submucosal cystic structures with peripheral foreign body and giant cell reaction
Disclosures:
Majd Aboona indicated no relevant financial relationships.
Erica Turse Dailey indicated no relevant financial relationships.
William Anderson indicated no relevant financial relationships.
Shifat Ahmed indicated no relevant financial relationships.
Majd Aboona, BS1, Erica Turse Dailey, DO, MPH2, William Anderson, MD2, Shifat Ahmed, MD2. E0109 - An Interesting Case of Pneumatosis Cystoides Intestinalis Diagnosed After Polypectomy: Case Report and Review of the Literature, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.