Sasikanth Ravi, DO1, Clive J. Miranda, DO2, Taylor Drake, MD3, Timothee Chapuis, DO1, Heather Arseneau, 4 1Abrazo Health Network, Glendale, AZ; 2University at Buffalo, Buffalo, NY; 3Abrazo Health Network, Goodyear, AZ; 4Arizona College of Osteopathic Medicine Midwestern, Glendale, AZ
Introduction: Rectal foreign bodies (RFB) present a unique management dilemma due to the variety of objects transanally impacted and their subsequent range of local trauma. A reluctance to seek medical assistance and present a candid recount of the incident can make diagnosis challenging and pose delays, further worsening the degree of injury before timely intervention can be provided. Consequently, our case aims to illustrate a systematic approach to the diagnosis and management of irretrievable rectal foreign bodies.
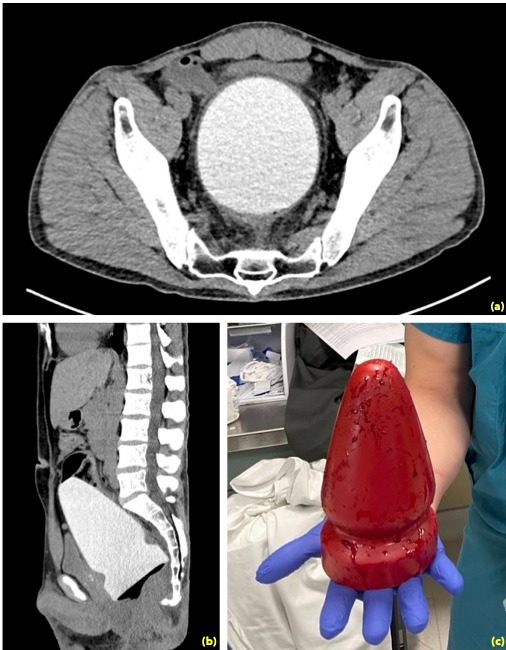
Case Description/Methods: The case illustrates a 45-year-old gentleman who presented to the ER with severe rectal pain. He reported that earlier in the day, he had felt adventurous and had self-inserted a rubber sex toy into his rectum. He had been unsuccessful in removing the toy despite multiple efforts and explained that, as time passed, he experienced worsening rectal pain with mild bleeding at the insertion site. Upon confirmation of a large palpable foreign body on the rectal exam, a computed tomography of the abdomen/pelvis showed a large triangular radiopaque foreign body within the rectum measuring 8.8 x 9.4 x 17.0 cm along with severe rectal wall thickening. The patient was immediately taken to the operating room where multiple attempts to transanally remove the impacted object were unsuccessful.This ultimately necessitated an exploratory laparotomy and colotomy with subsequent partial colectomy. An end colostomy was matured after field contamination from the spillage of colonic contents during the extraction of the foreign object.
Discussion: Rectal foreign bodies continue to be a clinical challenge with their increasing incidence. Although there is a predominance of RFBs in males, it is important to keep an impartial perspective. Notably, it is crucial to understand that RFBs are not limited to sexual satisfaction - but instead could be used for non-sexual purposes (i.e., packing of illicit drugs). Consequently, all RFBs need to be regarded as potentially hazardous. The presented case highlights the importance of a systematic approach which includes ruling out peritoneal signs via physical exam and imaging for potential evidence of perforation. Thereafter, it is important to attempt a manual and transanal removal of the RFB. If all approaches are unsuccessful, surgery via laparoscopy will be necessary. During surgery, the object can be "milked" toward the rectum to be removed transanally. If unsuccessful, however, a colotomy is imperative as illustrated in the presented case.
Figure: (a) CT Abdomen/Pelvis transverse view showing displaced anterior urinary bladder secondary to mass effect from the large rectal foreign body (b) Sagittal view of radiopaque foreign body within the rectum measuring 8.8 x 9.4 x 17.0 cm in greatest TV/AP/CC dimensions (c) Post-surgical removal after unsuccessful transanal extraction
Disclosures:
Sasikanth Ravi indicated no relevant financial relationships.
Clive Miranda indicated no relevant financial relationships.
Taylor Drake indicated no relevant financial relationships.
Timothee Chapuis indicated no relevant financial relationships.
Heather Arseneau indicated no relevant financial relationships.
Sasikanth Ravi, DO1, Clive J. Miranda, DO2, Taylor Drake, MD3, Timothee Chapuis, DO1, Heather Arseneau, 4. E0127 - Rectal Foreign Body Necessitating Surgical Intervention, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.