Kirk Kerkorian School of Medicine at UNLV Las Vegas, NV
Jose Aponte-Pieras, MD1, Nazanin Houshmand, MD1, Joseph Fayad, MD2, Irene H. Thung, MD3, Christian S. Jackson, MD4 1Kirk Kerkorian School of Medicine at UNLV, Las Vegas, NV; 2VA Southern Nevada Health Care System, Las Vegas, NV; 3Loma Linda VA Medical Center, Loma Linda, CA; 4VA Loma Linda Healthcare System, Loma Linda, CA
Introduction: Gastrointestinal neuroectodermal tumors (GNET) are a type of high-grade sarcoma of the gastrointestinal (GI) tract that share features with clear cell carcinoma of tendon sheaths and aponeuroses. Patients typically present with clinical signs and symptoms of small bowel obstruction, intussusception or abdominal mass. These tumors can arise in the stomach, colon, as well as metastasis to liver or regional lymph nodes. We present a case of ileal GNET in an otherwise asymptomatic patient with Iron-deficiency Anemia (IDA) diagnosed using video capsule endoscopy (VCE).
Case Description/Methods: A 58-year-old Hispanic male with a past medical history of GERD and obesity presented for evaluation of chronic microcytic anemia. Workup revealed: hemoglobin 8.6 g/dl, MCV 62.2, iron saturation 2.6%, transferrin 307 mg/dl, ferritin < 5 ng/ml, reticulocyte index of 1.34; serum folate, vitamin B12 and TSH levels were within normal limits. He was taking oral ferrous sulfate and vitamin C for IDA. He reported heartburn but denied melena, hematochezia, hematemesis, weight loss and had an unremarkable colonoscopy four years prior. Upper endoscopy revealed mild erosive esophagitis and mild chronic active gastritis with negative biopsies. Colonoscopy was unremarkable in the setting of optimal bowel preparation. VCE revealed an ulcerated mass occupying 35% of the ileal lumen. CT of the abdomen noted asymmetric wall thickening with enhancement of the small bowel. The patient underwent laparoscopy-assisted enteroscopy with rendezvous technique allowing direct visualization of a 3 cm proximal ileum mass requiring open segmental resection with primary anastomosis. Pathology suggested malignant GNET or clear cell sarcoma-like tumor of the GI tract. Immunohistochemistry was positive for neural crest markers (S100, SOX10) and Vimentin; negative for CD117, DOG1, HMB45, MART1, MAA, chromogranin, and synaptophysin. Fluorescence in-situ hybridization was positive for EWSR1 (22q12) rearrangement. Given the clear surgical margins, absent regional lymph node spread and lack of standard guidelines for this rare pT1N0M0 tumor, surveillance imaging every three months without adjuvant radiation or systemic chemotherapy was recommended.
Discussion: This case highlights the importance of VCE for small bowel assessment after negative bidirectional endoscopy to identify the etiology of IDA per American Gastroenterology Association guidelines. In this case, an ulcerated GNET was the etiology of IDA persisting despite iron supplementation.
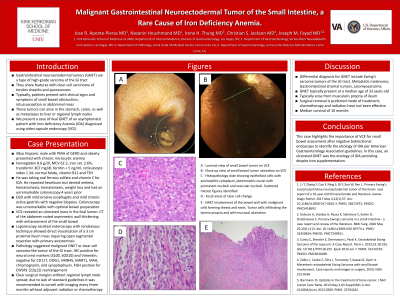
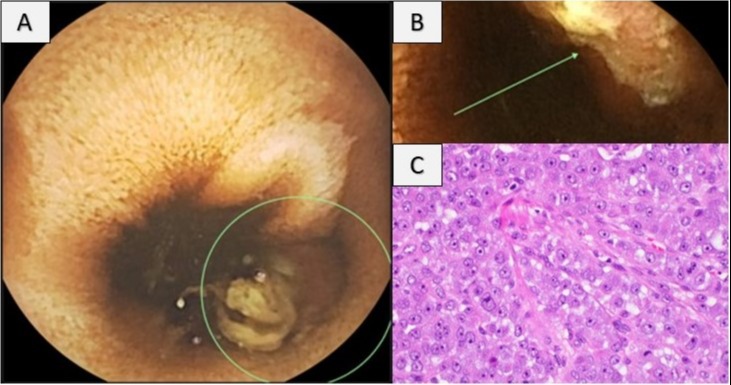
Figure: Figure 1A – Luminal view of small bowel tumor on Video Capsule Endoscopy (VCE) Figure 1B – Close up view of ulceration of small bowel tumor on VCE Figure 1C – Histopathology slide showing epithelioid cells with eosinophilic cytoplasm, pleomorphic nuclei with prominent nucleoli and vesicular nucleoli. Scattered mitotic figures identified.
Disclosures:
Jose Aponte-Pieras indicated no relevant financial relationships.
Nazanin Houshmand indicated no relevant financial relationships.
Joseph Fayad indicated no relevant financial relationships.
Irene Thung indicated no relevant financial relationships.
Christian Jackson indicated no relevant financial relationships.
Jose Aponte-Pieras, MD1, Nazanin Houshmand, MD1, Joseph Fayad, MD2, Irene H. Thung, MD3, Christian S. Jackson, MD4. A0644 - Malignant Gastrointestinal Neuroectodermal Tumor of the Small Intestine: A Rare Cause of Iron Deficiency Anemia, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.