New York-Presbyterian/Weill Cornell Medical Center New York, NY
Ariel Bar-Mashiah, MD1, David Wan, MD2 1New York-Presbyterian/Weill Cornell Medical Center, New York, NY; 2New York-Presbyterian Hospital/Weill Cornell Medicine, New York, NY
Introduction: Granular cell tumors (GCTs) are rare submucosal tumors of Schwann cell origin. These tumors are typically benign but have malignant potential in up to two percent of cases. GCTs are most commonly found in the oropharynx, skin, subcutaneous tissue, and breasts. If found in the gastrointestinal tract, they are most likely to be found in the middle to lower third of the esophagus. Due to the rarity of colonic GCTs, our understanding of these tumors is limited to case reports.
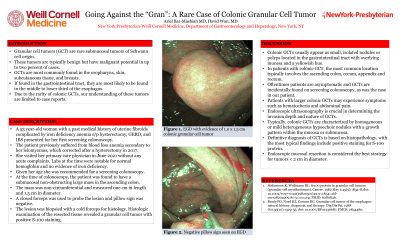
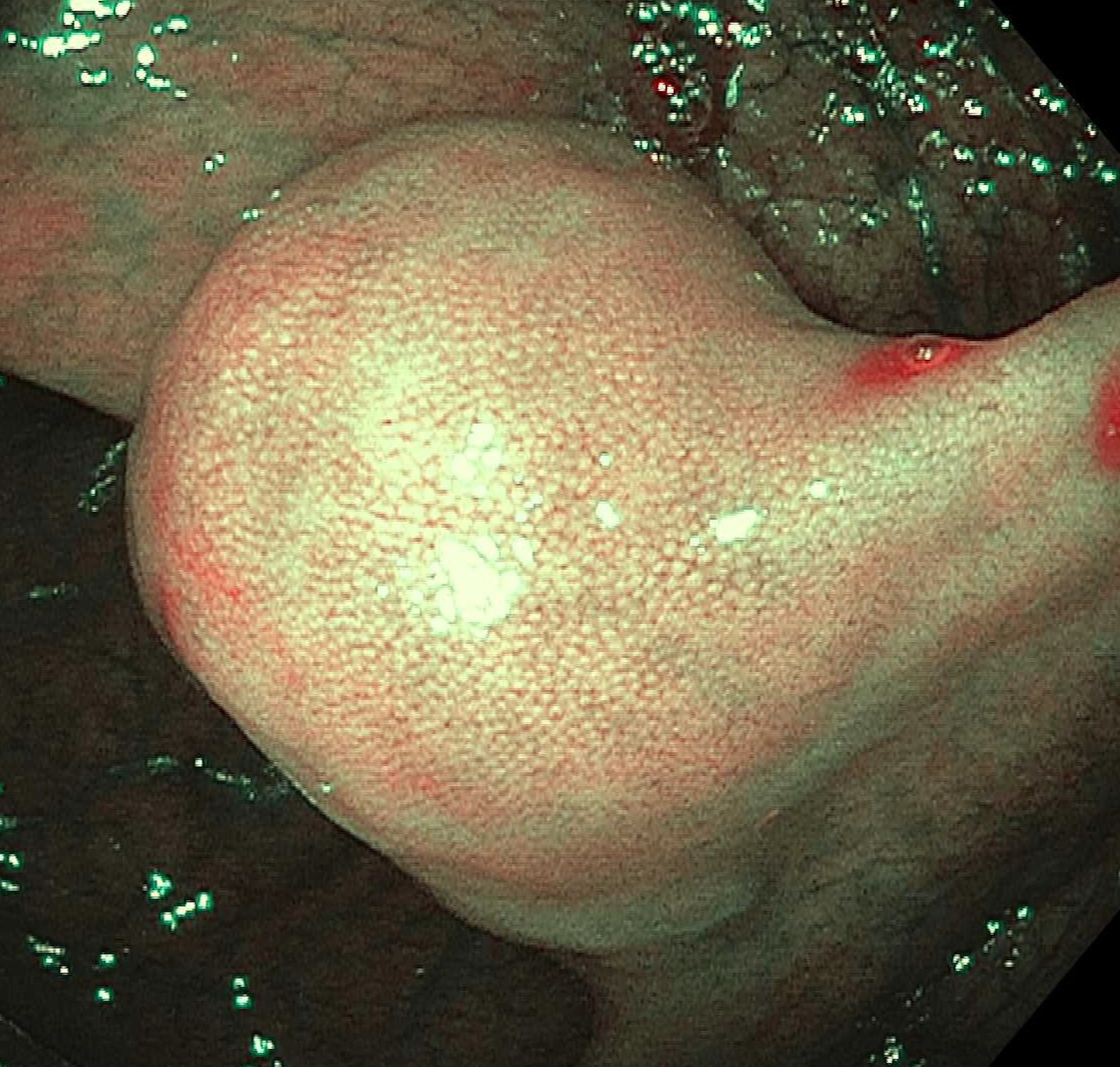
Case Description/Methods: A 53-year-old woman with a past medical history of uterine fibroids complicated by iron deficiency anemia status-post hysterectomy, GERD, and IBS presented for her first screening colonoscopy. The patient previously suffered from blood loss anemia secondary to her leiomyomas, which corrected after a hysterectomy in 2017. She visited her primary care physician in June 2021 without any acute complaints. Labs at the time were notable for normal hemoglobin and no evidence of iron deficiency. Given her age, she was recommended for a screening colonoscopy. At the time of colonoscopy, the patient was found to have a submucosal non-obstructing large mass in the ascending colon. The mass was non-circumferential and measured one cm in length and 1.5 cm in diameter. A closed forceps was used to probe the lesion and pillow sign was negative. The lesion was biopsied with a cold forceps for histology with a plan for further resection. Histologic examination of the resected tissue revealed a GCT with positive S-100 staining.
Discussion: Colonic GCTs usually appear as small, isolated nodules or polyps located in the gastrointestinal tract with overlying mucosa and a yellowish hue. In patients with colonic GCT, the most common location typically involves the ascending colon, cecum, appendix, and rectum. Oftentimes patients are asymptomatic and GCTs are incidentally found on screening colonoscopy, as was the case in our patient. Patients with larger colonic GCTs may experience symptoms such as hematochezia and abdominal pain. Endoscopic ultrasonography is crucial in determining the invasion depth and nature of GCTs. Typically, colonic GCTs are characterized by homogeneous or mild heterogeneous hypoechoic nodules with a growth pattern within the mucosa or submucosa. A definitive diagnosis of GCT is based on histopathology, with the most typical findings including positive staining for S-100 protein. Endoscopic mucosal resection is considered the best strategy for tumors < 2 cm in diameter.
Figure: Gross examination revealed a 1.0 x 1.5 cm mass with negative pillow sign
Disclosures:
Ariel Bar-Mashiah indicated no relevant financial relationships.
David Wan indicated no relevant financial relationships.
Ariel Bar-Mashiah, MD1, David Wan, MD2. A0156 - A Rare Case of Colonic Granular Cell Tumor, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.