New York Presbyterian Brooklyn Methodist Hospital, NY
Award: Presidential Poster Award
Megha Reddy, MD, Miguel Lacayo, MD, Michael Castillo, MD New York Presbyterian Brooklyn Methodist Hospital, Brooklyn, NY
Introduction: Eosinophilic gastrointestinal diseases (EGID) are immune-mediated conditions characterized by GI dysfunction and histological evidence of eosinophilic infiltration. While usually confined to the GI tract, severe inflammation can involve multiple organ systems, typically under the umbrella term of hypereosinophilic syndrome (HES). Patients can present with cardiac involvement such as eosinophilic myocarditis which results in an uncommon, but potentially lethal complication. We present a case of a patient with prior history of eosinophilic esophagitis (EoE) subsequently presenting with diffuse EGID complicated by eosinophilic myocarditis.
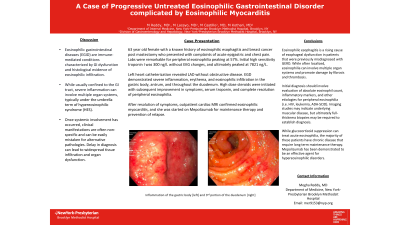
Case Description/Methods: A 63-year-old female with a history of EoE and breast cancer post mastectomy presented with acute epigastric and chest pain. The patient had biopsy-proven EoE which was managed with PPI in the past. On physical examination, she had diffuse abdominal tenderness. Labs were remarkable for peripheral eosinophilia peaking at 57%. Initial high sensitivity troponin I was 300 ng/L without EKG changes, and ultimately peaked at 7821 ng/L. CT of the abdomen and pelvis showed thickening of the stomach, duodenum, and jejunum. Left heart catheterization revealed LAD disease without obstructive disease. EGD demonstrated severe inflammation, erythema, and eosinophilic infiltration in the gastric body, antrum, and throughout the duodenum. High dose steroids were initiated with subsequent improvement in symptoms, serum troponin, and complete resolution of peripheral eosinophilia. Patient followed up as an outpatient, where cardiac MRI confirmed eosinophilic myocarditis, and she was started on Mepolizumab for maintenance therapy and prevention of relapse.
Discussion: EGID are increasingly prevalent disorders that can result in significant morbidity and mortality without prompt diagnosis. This patient had a history of EoE and developed diffuse GI involvement and subsequent eosinophilic myocarditis. Her presentation as atypical chest pain suggestive of NSTEMI resulted in delay of initiation of steroids until after heart catheterization. Our case suggests that without glucocorticoid suppression, eosinophilia can cause widespread tissue infiltration and damage. The majority of these patients have chronic disease that require long term maintenance therapy. Mepolizumab has been demonstrated to be an effective agent for hypereosinophilic disorders. When managing EGID, it is pertinent to recognize early involvement of systemic eosinophilic infiltration.
Figure: EGD
Disclosures:
Megha Reddy indicated no relevant financial relationships.
Miguel Lacayo indicated no relevant financial relationships.
Michael Castillo indicated no relevant financial relationships.
Megha Reddy, MD, Miguel Lacayo, MD, Michael Castillo, MD. E0246 - A Case of Progressive Untreated Eosinophilic Gastrointestinal Disorder Complicated by Eosinophilic Myocarditis, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.