University of Alabama at Birmingham School of Medicine Birmingham, AL
Kathryn Reynolds, MS, MPH1, Ryan LaGrange, MD2, Amanda Cartee, MD2 1University of Alabama at Birmingham School of Medicine, Birmingham, AL; 2University of Alabama at Birmingham, Birmingham, AL
Introduction: Chronic intestinal pseudo-obstruction (CIPO) is a rare motility disorder with a variety of secondary causes, including genetics, metabolic disease, paraneoplastic syndromes, inflammatory disorders, and neurologic disorders. We present a case of CIPO secondary to pelvic floor dyssynergia.
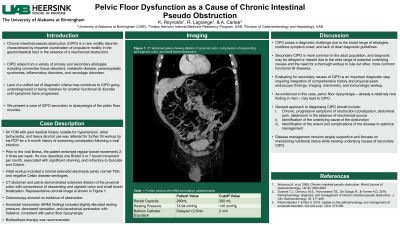
Case Description/Methods: A 64 year-old male with a past medical history of hypertension, atrial tachycardia, and heavy alcohol use was referred for further GI workup by his primary care physician following a five month history of worsening constipation after a viral infection. Prior to the infection, he had a bowel movement 2-3 times per week. However, he now describes one Bristol 4 or 7 bowel movement with straining per month. Symptoms were refractory to Dulcolax and Colace. Initial workup included a normal extended electrolyte panel, normal TSH, and negative Celiac disease serologies. A CT abdomen and pelvis revealed extensive dilation of proximal colon, compression of descending and sigmoid colon, and small bowel fecalization. A representative coronal image is shown in Figure 1. Subsequent colonoscopy did not reveal any evidence of obstruction. Anorectal manometry (ARM) findings included elevated resting pressure (74.94 mmHg), decreased sensation, paradoxical contraction with Valsalva, and inability to pass the balloon catheter after 2.5 minutes. Normal rectal capacity (280 mL) and excellent squeeze pressure but paradoxical contraction with Valsalva is consistent with pelvic floor dyssynergia. Biofeedback therapy was recommended.
Discussion: Evaluating for secondary causes of CIPO (i.e., obstruction, metabolic disturbances, autoimmune disorders, neurologic disorders, and musculoskeletal disorders) is an important diagnostic step. Key tests include imaging, colonoscopy, electrolytes and autoimmune panels, and anorectal manometry. This case highlights long-standing pelvic floor dyssynergia as an underlying cause of CIPO.
Figure: Figure 1 - CT abdomen and pelvis with extensive dilation of proximal colon and small bowel fecalization
Disclosures:
Kathryn Reynolds indicated no relevant financial relationships.
Ryan LaGrange indicated no relevant financial relationships.
Kathryn Reynolds, MS, MPH1, Ryan LaGrange, MD2, Amanda Cartee, MD2. E0270 - Pelvic Floor Dysfunction as a Cause of Chronic Intestinal Pseudo Obstruction, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.