University of Rochester Medical Center Rochester, NY
Sarah Enslin, PA-C1, Muhammad Waqas Tahir, MD2, Raseen Tariq, MD3, Vivek Kaul, MD, FACG1 1University of Rochester Medical Center, Rochester, NY; 2Rochester General Hospital, Rochester, NY; 3Mayo Clinic, Rochester, MN
Introduction: Neuroendocrine tumors (NET) most commonly develop in the lungs, appendix, bowel and pancreas. Esophageal NET is extremely rare, comprising < 2% of all NETs. The most common symptom is dysphagia although patients may be asymptomatic. We present a case of metastatic esophageal NET and a literature review.
Case Description/Methods: A 61-year-old female with 5-month history of progressively worsening chest tightness, weight loss and diarrhea underwent abdominal CT scan which revealed enlarged gastrohepatic lymph nodes (LN). EGD showed a 3cm ulcerated lesion at the gastroesophageal junction (GEJ). Biopsies suggested high-grade NET in the background of high-grade dysplasia. PET/CT confirmed a 3.0 x 2.3cm ill-defined, hypermetabolic, soft tissue mass at the GEJ (SUV max 9.0) and several hypermetabolic, enlarged gastrohepatic LNs, largest measuring 2.8 x 2.0cm (SUV max 8).
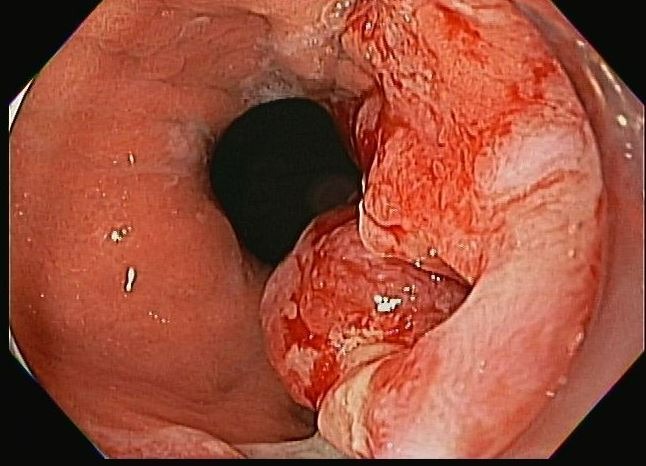
The patient was referred to our center for further management. Repeat EGD revealed a 3cm distal esophageal lesion with central ulceration extending across the GEJ into the high cardia (Image 1). On endoscopic ultrasound (EUS), a hypoechoic mass is seen with involvement of the muscularis propria (T2). Peri-gastric lymphadenopathy was present. Transgastric fine needle aspiration (FNA) of the largest LN confirmed metastatic neuroendocrine tumor (T3N1). Repeat endoluminal biopsies from the esophageal lesion confirmed poorly-differentiated NET, CD56 and synaptophysin positive, Ki-67 > 90%. Multidisciplinary tumor board recommended chemotherapy with carboplatin and etoposide. No evidence of disease progression noted after the first 3 cycles; patient remains on treatment.
Discussion: Metastatic poorly-differentiated high-grade NET of the esophagus is very rare. First-line therapy is chemotherapy. Average prognosis with treatment is 12-18 months. Immunotherapy may provide additional survival benefit however data is extremely limited so this is typically reserved for second-line therapy (if progression on chemotherapy). Given the rarity and aggressiveness of these lesions, accurate pathological diagnosis and multidisciplinary discussion is critical for optimal management of these patients.
References:
1. Giannetta E, Guarnotta V, Rota F, et al. A rare rarity: neuroendocrine tumor of the esophagus. Crit Rev Oncol Hematol. 2019;137:92-107
2. Lee C, Lim Y, Park S, et al. The clinical features and treatment modality of esophageal neuroendocrine tumors: a multicenter study in Korea. BMC Cancer. 2014; 14:569.
Figure: Image 1: large distal esophageal lesion with central ulceration
Disclosures:
Sarah Enslin indicated no relevant financial relationships.
Muhammad Waqas Tahir indicated no relevant financial relationships.
Raseen Tariq indicated no relevant financial relationships.
Vivek Kaul: Ambu – Consultant. CDX – Consultant. Cook Medical – Consultant. Motus GI – Consultant. Steris Corp – Consultant.
Sarah Enslin, PA-C1, Muhammad Waqas Tahir, MD2, Raseen Tariq, MD3, Vivek Kaul, MD, FACG1. D0229 - Metastatic, Poorly-Differentiated Neuroendocrine Tumor of the Esophagus: Case Report and Literature Review of a “Rare Rarity”!, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.