New York Presbyterian Brooklyn Methodist Brooklyn, NY
Dean Rizzi, MD1, Michael Liben, MD2, Harsh Patel, MD, MPH2, Daniel Golpanian, MD3, Navim Mobin, MD2, Michael Castillo, MD3, Amar Manvar, MD3 1New York Presbyterian Brooklyn Methodist, Brooklyn, NY; 2NewYork Presbyterian Brooklyn Methodist Hospital, Brooklyn, NY; 3New York Presbyterian Brooklyn Methodist Hospital, Brooklyn, NY
Introduction: Percutaneous Endoscopic Gastrostomy (PEG) is the creation of external access to the stomach bypassing the enteral pathway in order to provide medications and nutrition. Alternatives to endoscopic gastrostomy tube placement include surgical or radiographically placed gastrostomy tubes individual anatomic and clinical circumstances. Buried Bumper Syndrome (BBS), is a well known late complication of PEG tube placement and occurs due to the tight apposition of the external bolster against the abdominal wall creating traction on the internal bolster, resulting in gastric erosion. Incidence of BBS is estimated to be about 0.3%-2.4% and can recur multiple times even after correction.
Case Description/Methods: We report a case of an 83 year old man with a history of Pallister Killian Syndrome, aortic stenosis, atrial fibrillation and asthma. The patient presented to the emergency department for the evaluation of a dislodged PEG tube and peristomal cellulitis 4 weeks after PEG tube placement at another hospital. An abdominal CT scan revealed evidence of BBS with a large hiatal hernia associated with partial intrathoracic stomach without evidence of gastric volvulus. The PEG tube was removed and after resolution of peristomal cellulitis, and a new PEG tube was placed. On post procedure day 2, the patient began to develop progressive abdominal distension and pain. A repeat abdominal CT scan demonstrated recurrent BBS. A subsequent fluoroscopic tube study showed immediate intra-abdominal extravasation of contrast. The patient then underwent laparoscopic hiatal hernia reduction with anterior gastropexy and surgical jejunostomy placement.
Discussion: Literature for early BBS is sparse, with few cases reported. On review, early BBS has been reported in patients on chemotherapy or with pre-procedural cachexia. It is likely that chemotherapeutic destruction of mucosal tissue and poor wound healing may accelerate gastric erosion leading to early BBS. PEG placement has long been thought of as a means to prevent paraesophageal hernias. The fixation of the stomach at the greater curvature should prevent proximal movement of the gastrointestinal tract at the level of the diaphragm. As seen in our case, it is possible that continued cephalad movement of the large hernia may have placed significant traction on the internal bumper resulting in recurrent early BBS. We hypothesize that large paraesophageal hernia may be a risk factor for early BBS and gastropexy should be considered during initial PEG placement.
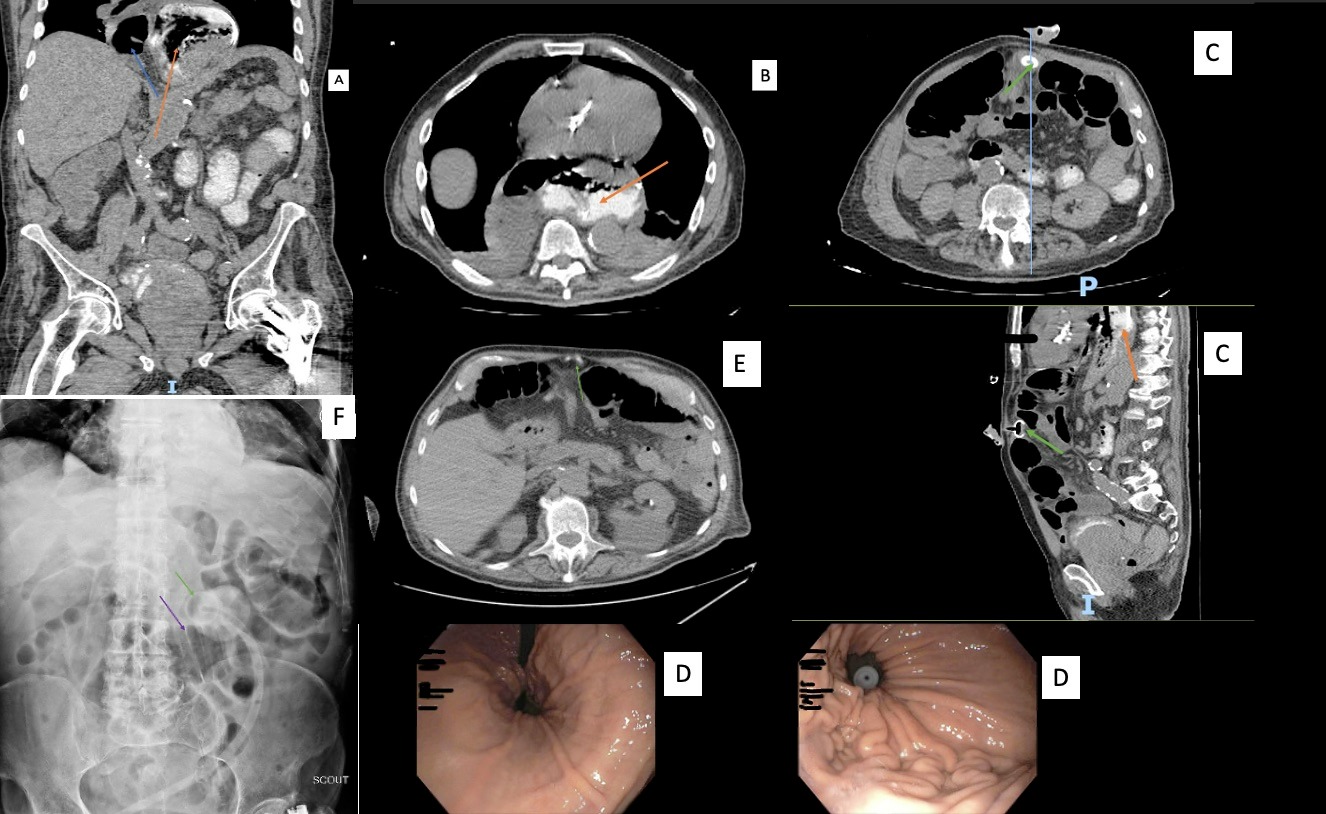
Figure: Figure: (A) orange arrow showing intrathoracic transposition of stomach and blue arrow showing intrathoracic loop of small bowel. (B) orange arrow showing intrathoracic transposition of stomach. (C) (linked sagittal and coronal CT) green arrow showing internal bumper terminating within fibrinous, orange arrow showing intrathoracic stomach. (D) endoscopic visualization of hiatal hernia and internal bumper. (E) green arrow denoting internal bumper with surrounding edema in ventral abdominal wall. (F), (FL tube study) purple arrow showing intra abdominal contrast extravasation and green arrow showing bumper.
Disclosures:
Dean Rizzi indicated no relevant financial relationships.
Michael Liben indicated no relevant financial relationships.
Harsh Patel indicated no relevant financial relationships.
Daniel Golpanian indicated no relevant financial relationships.
Navim Mobin indicated no relevant financial relationships.
Michael Castillo indicated no relevant financial relationships.
Amar Manvar indicated no relevant financial relationships.
Dean Rizzi, MD1, Michael Liben, MD2, Harsh Patel, MD, MPH2, Daniel Golpanian, MD3, Navim Mobin, MD2, Michael Castillo, MD3, Amar Manvar, MD3. D0469 - Recurrent Early Buried Bumper Syndrome in Context of Large Paraesophageal Hernia, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.