David Wozny, DO1, Christopher Dipollina, DO1, Jaimy Villavicencio Kim, MD2, Murali Dharan, MD, MRCP3 1University of Connecticut, Farmington, CT; 2UConn Health, Farmington, CT; 3University of Connecticut, Hartford, CT
Introduction: In rare circumstances, pleural fluid can accumulate from outside of the blood vessels. This disease state has been termed pleural effusion of extra-vascular origin (PEEVO) and can include urine, CSF, bile, dialysate or chyle. We present a case of spontaneous translocation of bile into the thorax in a patient with a hepatic duct stricture.
Case Description/Methods: An 88-year-old male with history of cholecystitis status post cholecystectomy complicated by common hepatic duct stricture with indwelling T-tube presented with two days of fatigue, abdominal pain and shortness of breath. Prior to presentation, the T-tube was functional for several months and then was removed inadvertently while at home. CT of the abdomen showed intracapsular fluid collection along the posteroinferior liver and right sided pleural effusion. MRCP showed CBD stricture with intrahepatic ductal dilatation. ERCP was performed and the proximal biliary tree was unable to be opacified with contrast. A percutaneous trans-biliary drain was placed with fluid samples positive for staph simulans. Repeat ERCP was performed, and two stents were placed in the common bile duct.
A repeat CT scan showed an interval increase in both the size of the hepatic subcapsular fluid collection and the pleural effusion. A chest tube was placed and 1.5L of green fluid was removed. Fluid studies showed WBC 925, glucose 54, LDH 1831k, protein 2.9, Bilirubin 7.5 (serum bilirubin 0.8), and pH 7.21. The diagnosis of bilothorax was made. Repeat imaging demonstrated improvement in fluid collection and the chest tube was removed after 5 days.
Discussion: PEEVO in which bile is the accumulated fluid is termed as “bilothorax” and is often the result of injury to the biliary tree leading to a fistula between the tree and pleural space. In this case, there was spontaneous translocation of bile which is quite uncommon. Imaging will demonstrate isolated right-sided pleural effusion. Diagnosis is confirmed with fluid studies, the effusion is often exudative, and the distinguishing feature is the presence of bilirubin in the fluid. If the bilirubin concentration in the pleural fluid is greater than that of the serum bilirubin, the diagnosis of bilothorax is made. Coordination between pulmonology and gastroenterology specialists is essential for prompt drainage of the accumulation and decompression of the biliary system. The presence of a fistula would additionally warrant surgical correction.
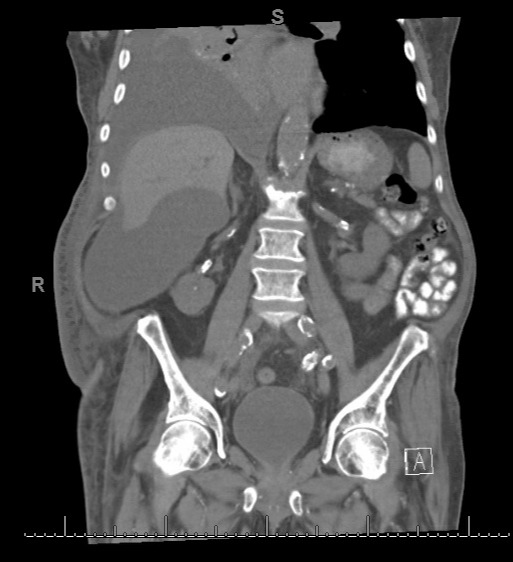
Figure: CT Abdomen demonstrating sub-capsular fluid collection with expansion into right pleural space
Disclosures:
David Wozny indicated no relevant financial relationships.
Christopher Dipollina indicated no relevant financial relationships.
Jaimy Villavicencio Kim indicated no relevant financial relationships.
Murali Dharan indicated no relevant financial relationships.
David Wozny, DO1, Christopher Dipollina, DO1, Jaimy Villavicencio Kim, MD2, Murali Dharan, MD, MRCP3. D0079 - Bilothorax: Uncommon Accumulation in the Pleural Space, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.