Jordan C. Malone, DO1, Giri Movva, BS2, Anni Chowdhury, DO1, Nikita Prasad, MD1, Jaison John, MD1, Manav S. Sharma, MD1 1University of Texas Medical Branch, Galveston, TX; 2John Sealy School of Medicine, University of Texas Medical Branch, Galveston, TX
Introduction: AIDS cholangiopathy is a rare biliary tract syndrome seen in AIDS patients primarily with CD4 counts less than 100 cells/microliter. It commonly manifests as multiple biliary strictures secondary to chronic inflammation caused by one or more opportunistic infectious pathogens with Cryptosporidium parvum being isolated in most cases. The overall incidence is currently unknown but has decreased since initiation of potent ART in the mid-1990s. Here we describe a case of a 29-year-old male with newly diagnosed AIDS who presented with months of gradually worsening abdominal pain and diarrhea.
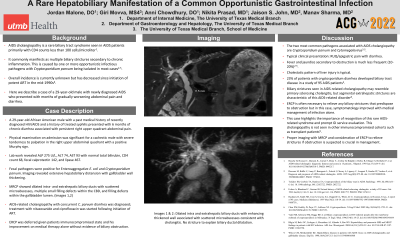
Case Description/Methods: A 29-year-old African American man with a past medical history of recently diagnosed HIV/AIDS and treated syphilis presented with 6 months of chronic diarrhea associated with persistent right upper quadrant abdominal pain. Physical examination on admission was significant for a cachectic male with severe tenderness to palpation in the right upper abdominal quadrant with a positive Murphy sign. Lab work revealed ALP 275 U/L, ALT 74, AST 93 with normal total bilirubin, CD4 count 68, fecal calprotectin 142, and lipase 467. Fecal pathogens were positive for Enteroaggregative Escherichia coli and Cryptosporidium parvum. Imaging revealed extensive hepatobiliary distension with gallbladder wall thickening. MRCP showed dilated intra- and extrahepatic biliary ducts with scattered microabscesses, multiple small filling defects within the CBD, and filling defects within the gallbladder lumen. AIDS-related cholangiopathy was diagnosed and treatment with nitazoxanide and ciprofloxacin was started following initiation of ART. ERCP was deferred given the patient's immunocompromised state and his improvement on medical therapy alone without evidence of biliary obstruction.
Discussion: The two most common pathogens associated with AIDS cholangiopathy are Cryptosporidium parvum and Cytomegalovirus. ERCP is often necessary to relieve any biliary strictures that predispose to obstruction but in this case, symptomatology improved with medical management of infection alone. This case highlights the importance of recognition of this rare AIDS-related syndrome and prompt GI service evaluation as this cholangiopathy is not seen in other immunocompromised cohorts such as transplant patients. Proper imaging with MRCP and consideration of ERCP to relieve strictures if obstruction is suspected is crucial.
Figure: MRCP findings
Disclosures:
Jordan Malone indicated no relevant financial relationships.
Giri Movva indicated no relevant financial relationships.
Anni Chowdhury indicated no relevant financial relationships.
Nikita Prasad indicated no relevant financial relationships.
Jaison John indicated no relevant financial relationships.
Manav Sharma indicated no relevant financial relationships.
Jordan C. Malone, DO1, Giri Movva, BS2, Anni Chowdhury, DO1, Nikita Prasad, MD1, Jaison John, MD1, Manav S. Sharma, MD1. E0064 - A Rare Hepatobiliary Manifestation of a Common Opportunistic Gastrointestinal Infection, ACG 2022 Annual Scientific Meeting Abstracts. Charlotte, NC: American College of Gastroenterology.