Eric Prado, MD1, Yasi Xiao, MDCM2, Ankita Tirath, MD1, Carl L. Kay, MD3, Mithun Sharma, MD4, Giada Sebastiani, MD5, Matthew Ciorba, MD1, Nicholas Davidson, MD1, Anish Patel, DO6, Talat Bessisow, MD, MSc5, Rupa Banerjee, DTM, MD, MRCP4, Scott McHenry, MD1, Parakkal Deepak, MBBS, MS1 1Washington University in St. Louis, St. Louis, MO; 2University of Toronto, Toronto, ON, Canada; 3Brooke Army Medical Center, JBSA Fort Sam Houston, TX; 4Asian Institute of Gastroenterology, Hyderabad, Telangana, India; 5McGill University Health Centre, Montreal, PQ, Canada; 6Brooke Army Medical Center, Fort Sam Houston, TX
Introduction: Crohn’s Disease (CD) patients are twice as likely compared to controls to develop nonalcoholic fatty liver disease (NAFLD) leading to increased risk of cardiometabolic complications. Given this, we developed the first clinical screening tool for NAFLD in CD, Clinical Predictor for NAFLD in CD (CPN-CD) which uses readily accessible laboratory and clinical parameters. We have demonstrated CPN-CD outperforms the Hepatic Steatosis Index in detecting NAFLD in CD in an internal cohort. Here we performed a multicenter analysis to externally validate CPN-CD against transient elastography (TE) and establish its diagnostic accuracy to detect NAFLD in patients with CD at two different controlled attenuation parameter (CAP) thresholds.
Methods: A total of 454 patients with CD across four prospective cohorts from tertiary IBD centers across United States, Canada and India were included in the study. Of these, 412 patients were screened with TE only to determine prevalence of hepatic steatosis while 42 were screened with additional gold standard magnetic resonance imaging derived proton density fat fraction (MRI-PDFF), where hepatic steatosis was defined as ≥ 5.5% fat density, then reflexed to TE. To evaluate discriminative ability of CPN-CD to screen for NAFLD, patients were split into two CAP categories on TE; CAP ≥ 248 dB/m or ≥ 300 dB/m.
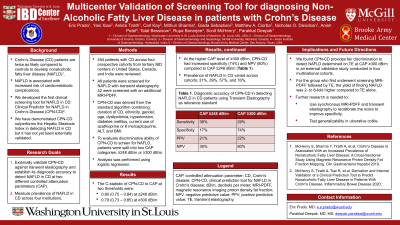
Results: In the four cohorts, the prevalence of NAFLD ranged from 32% to 76%. Using logistic regression, the relationship of CPN-CD to CAP ≥ 248 dB/m and CAP ≥ 300 dB/m revealed C-statistic 0.80 (0.75 – 0.84) and 0.79 (0.73 – 0.85) respectively. However, at CAP ≥ 300 dB/m, CPN-CD had higher specificity (74%) and NPV (80%) compared to CAP ≥ 248 dB/m (Table 1). For the group who first underwent screening MRI-PDFF the yield of finding NAFLD was 2- to 6-fold higher compared to TE alone.
Discussion: CPN-CD provides fair discrimination to detect NAFLD determined on TE at CAP ≥ 300 dB/m in an external validation study conducted in four multinational cohorts. Future directions include synchronous MRI-PDFF and TE to recalibrate the score to improve specificity and then test generalizability in ulcerative colitis.
CAP ≥ 248 dB/m
CAP ≥ 300 dB/m
Sensitivity
36%
29%
Specificity
17%
74%
PPV
21%
22%
NPV
30%
80%
Table: Table 1. Diagnostic accuracy of CPN-CD in detecting NAFLD in CD patients using transient elastography as reference standard.